Revisión teparia antiagregante plaquetaria post Sindrome Coronario Agudo
13
Long-term antiplatelet therapy after coronary artery stenting in stable patients Donald Cutlip, MD Jose C Nicolau, MD, PhD, FACC Uptodate Last updated: Feb 25, 2016. Juan J. Araya C. Interno Medicina Interna – Universidad de Antofagasta Módulo Cardiología
-
Upload
juan-jose-araya-cortes -
Category
Health & Medicine
-
view
181 -
download
1
Transcript of Revisión teparia antiagregante plaquetaria post Sindrome Coronario Agudo
Long-term antiplatelet therapy after coronary artery stenting in stable patients
Donald Cutlip, MDJose C Nicolau, MD, PhD, FACC
UptodateLast updated: Feb 25, 2016.
Juan J. Araya C.
Interno Medicina Interna – Universidad de Antofagasta
Módulo Cardiología
Duration Patients with stable coronary artery disease who have undergone
percutaneous coronary intervention (PCI) with stenting (either bare metal stent [BMS] or drug-eluting stent [DES]), we recommend aspirin 75 to 100 mg daily plus clopidogrel 75 mg daily for at least 12 months.
who have tolerated this therapy, additional 18 months.
With high bleeding risk less than 1 year of DAPT – a history of ischemic attack or stroke
– age ≥75 years, propensity to bleed (eg, recent trauma or surgery, recent or recurrent gastrointestinal bleeding, active peptic ulcer disease, severe hepatic impairment),
– body weight <60 kg,
– oral anticoagulants or nonsteroidal antiinflammatory drugs [NSAIDs]
Occasionally, patients may unexpectedly need to stop DAPT prior to 12 months. – the “minimum” duration of uninterrupted terapy
is 30 days.
If a bleeding event occurs or the bleeding risk is high, we consider limiting therapy to as short as 1 month in some cases. (the risk of stent thrombosis with BMS is greatest in the first 14 to 30 days)
Duration
For patients who have successfully completed 1 year of DAPT, discuss with them benefits and risks of continuing therapy
DAPT SCORE:– score of <2 stop at 12 months.
– Score >= 2 continue therapy for an additional 18 months
To be used in conjunction with clinical judgement.
Duration
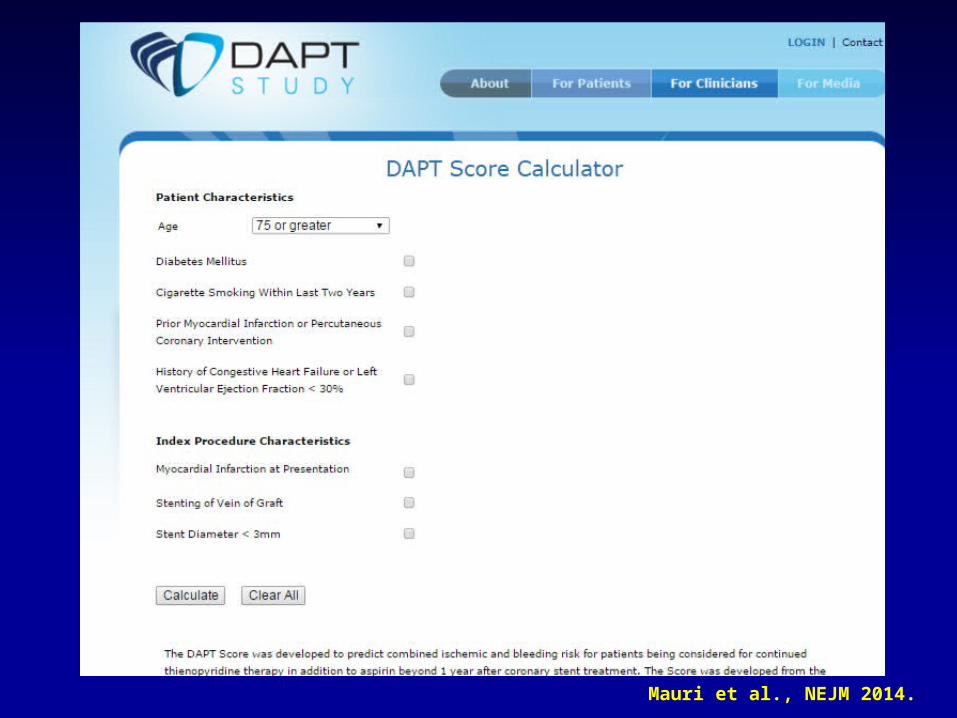
Mauri et al., NEJM 2014.
A 2015 meta-analysis (nine trials including 29,531 patients), which is representative, found the following comparing longer- with shorter-duration DAPT :
– A lower risk for MI (risk ratio [RR] 0.73, 95% CI 0.58-0.92). This represents 8 fewer MIs per 1000 treated patients per year.
– A higher risk for major bleeding (RR 1.63, 95% CI 1.34-1.99). This represents 6 more major bleeds per 1000 patients treated per year.
Duration
Bare metal stents:
– For patients who have received BMS, our recommendations are the same as for DES.
– The DAPT trial provided evidence to suggest that the benefit for prolonged DAPT is largely independent of stent type.
ACS treated medically (no PCI):
– DAPT, compared with aspirin alone, reduces the rate of MI
Duration
SUMMARY AND RECOMMENDATIONS The risk of coronary artery stent thrombosis and its consequences
of myocardial infarction (MI) or death are diminished by the use of dual antiplatelet therapy (DAPT) with aspirin and a platelet P2Y12 receptor blocker compared with the use of aspirin monotherapy.
Stable patients with (DES/BMS) not at high bleeding risk and who do not have planned noncardiac surgery within one year, least 12 months (1B).
1 year of successful DAPT therapy, discuss benefits and risks of continuing DAPT.
– use the DAPT score to aid in decision-making.
If during the first 12 months not had a significant complication additional 18 months (Grade 2B).
It is reasonable for patients to decide to stop DAPT after 12 months if they are particularly concerned about the increased risk of death or bleeding or due to a hardship associated with continuing DAPT.
SUMMARY AND RECOMMENDATIONS (2)
BMS patients at high bleeding risk or who have planned noncardiac surgery within one year, minimum of 1 month of uninterrupted DAPT (Grade 1B).
DES patients uninterrupted DAPT for a minimum of 6 months (Grade 1B).
We recommend continuing aspirin indefinitely in all stented patients (Grade 1A).
SUMMARY AND RECOMMENDATIONS (3)
ACC/AHA2014
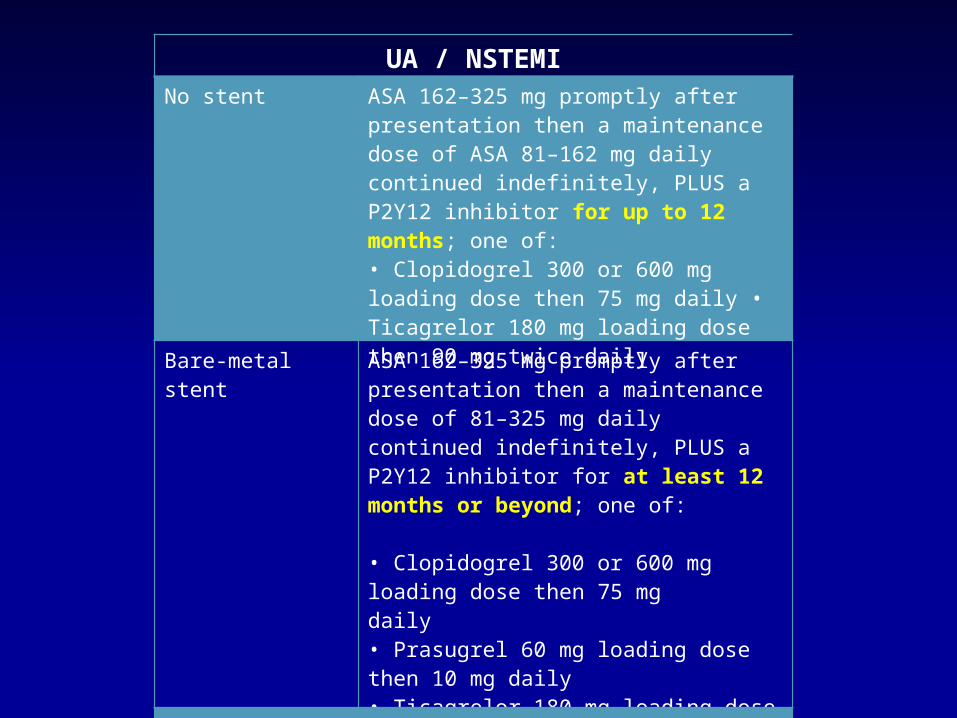
UA / NSTEMINo stent ASA 162–325 mg promptly after
presentation then a maintenance dose of ASA 81–162 mg daily continued indefinitely, PLUS a P2Y12 inhibitor for up to 12 months; one of: • Clopidogrel 300 or 600 mg loading dose then 75 mg daily • Ticagrelor 180 mg loading dose then 90 mg twice daily
Bare-metal stent ASA 162–325 mg promptly afterpresentation then a maintenance dose of 81–325 mg daily continued indefinitely, PLUS a P2Y12 inhibitor for at least 12 months or beyond; one of:
• Clopidogrel 300 or 600 mg loading dose then 75 mgdaily• Prasugrel 60 mg loading dose then 10 mg daily• Ticagrelor 180 mg loading dose then 90 mg twice daily
Drug-eluting stent As for bare-metal stent
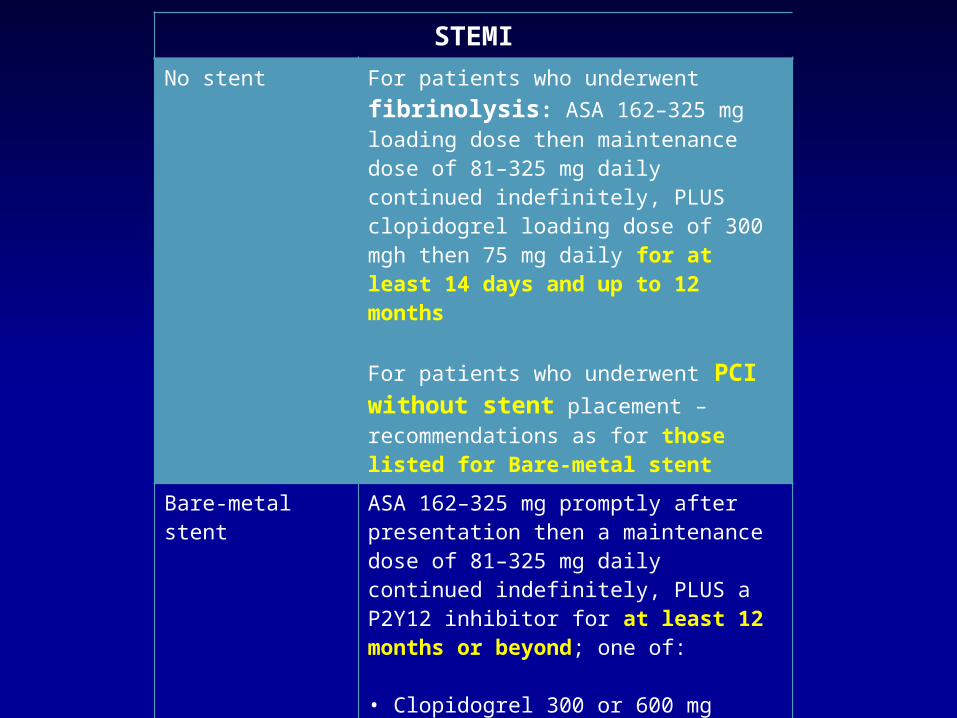
STEMINo stent For patients who underwent fibrinolysis:
ASA 162–325 mg loading dose then maintenance dose of 81–325 mg daily continued indefinitely, PLUS clopidogrel loading dose of 300 mgh then 75 mg daily for at least 14 days and up to 12 months
For patients who underwent PCI without stent placement – recommendations as for those listed for Bare-metal stent
Bare-metal stent ASA 162–325 mg promptly after presentation then a maintenance dose of 81–325 mg daily continued indefinitely, PLUS a P2Y12 inhibitor for at least 12 months or beyond; one of:
• Clopidogrel 300 or 600 mg loading dose then 75 mg daily• Prasugrel 60 mg loading dose then 10 mg daily• Ticagrelor 180 mg loading dose then 90 mg twice daily
Drug-eluting stent As for bare-metal stent