Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia
4
Med Oral Patol Oral Cir Bucal. 2011 Jul 1;1 6 (4):e537-40. Submandi bular gland aplasia with subling ual gland hyper trophy e537 Journal section: Oral Surgery Publication Types: Review Unilateral submandibular gland aplasia with ipsilateral sublingual gland hypertrophy presenting as a neck mass Gonzalo Herrera-Calvo 1 , Belén García-Montesinos-Perea 2 , Ramón Saiz-Bustillo 3 , Jaime Gallo-Te rán 4 , Pe- dro Lastra-García-Barón 5 1 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esi- Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esi- dent 2 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). t- Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). t- tending Surgeon 3 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). ead o epartment 4 eparment o a diodiology . ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esident 5 eparment o adiodiology. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). Sta radiologist Correspondence: Hospital Universitario Marqués de Valdecilla Servicio de Cirugía Oral y Maxilofacial Avenida de Valdecilla 25 39008 Santander (Cantabria) Spain [email protected] eceied: 27/02/2010 ccepted: 08/04/2010 Abstract The congenital absence o the major saliary glands is a ery inreuent disorder� in which seeral glands are usu- ally inoled at the same time. Sometimes this disorder can be associated with other deelopmental anomalies. The unilateral aplasia of the submandibular gland is an extremely rare nding with only 14 cases reported in the literat ure. Clinically, this kind of patients may complain of dry ness of the mouth, difculties in chewing and swal - lowing� seere periodontal disease or multiple caries� but usually they ollow an asymptomatic course. Saliary gland aplasia can be diagnosed with a large ariety o imaging techniues� which include computer tomography (CT)� magnetic resonance imaging (M)� ultrasonography (S)� sialography� or scintigraphy. In this paper we repor t a case o a patient re erred t o our depar tment with a long term a nd progressie growing neck mass� who has an unilateral submandibular gland aplasia associated to an ipsilateral hypertrophy o the sublingual gland. Key words: Submandibular gland aplasia, sublingual gland hypertrophy, neck mass. errera-Calo G� García-Montesinos-Perea B� Saiz-Bustillo � Gallo- Terán J� Lastra-García-Barón P. nilateral submandibular gland aplasia with ipsilateral sublingual gland hypertrophy presenting as a neck mass. Med Or al Patol Oral Cir Bucal . 2011 Jul 1;1 6 (4):e5 37-40. http://www.medicinaoral.com/medoralree01/16i4/medoral16i4p537.pd Article Number: 16895 http://www .medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Inde Epanded Journal Citation eports Inde Medicus� MELINE� PubMed Scopus� Embase and Emcare Indice Mdico Español doi:10.4317/medoral.16.e537 http://dx.doi.org/doi:10.4317/medoral.16.e537
-
Upload
jian-sian-li -
Category
Documents
-
view
221 -
download
0
Transcript of Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia

8/6/2019 Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia
http://slidepdf.com/reader/full/ref-6-herrera-2011-unilateral-sub-mandibular-gland-aplasia 1/4
Med Oral Patol Oral Cir Bucal. 2011 Jul 1;16 (4):e537-40. Submandi bular gland aplasia with subling ual gland hyper trophy
e537
Journal section: Oral Surgery
Publication Types: Review
Unilateral submandibular gland aplasia with ipsilateral sublingual
gland hypertrophy presenting as a neck mass
Gonzalo Herrera-Calvo 1, Belén García-Montesinos-Perea 2, Ramón Saiz-Bustillo 3, Jaime Gallo-Terán 4, Pe-
dro Lastra-García-Barón 5
1 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esi-Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esi-
dent2 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). t-Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). t-
tending Surgeon3 Oral and Mailoacial Surgery epartment. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). ead
o epartment4
eparment o adiodiology. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). esident5 eparment o adiodiology. ospital niersitario Marus de aldecilla� Santander (Cantabria� Spain). Sta radiologist
Correspondence:
Hospital Universitario Marqués de Valdecilla
Servicio de Cirugía Oral y Maxilofacial
Avenida de Valdecilla 25
39008 Santander (Cantabria) Spain
eceied: 27/02/2010
ccepted: 08/04/2010
AbstractThe congenital absence o the major saliary glands is a ery inreuent disorder� in which seeral glands are usu-
ally inoled at the same time. Sometimes this disorder can be associated with other deelopmental anomalies.
The unilateral aplasia of the submandibular gland is an extremely rare nding with only 14 cases reported in the
literature. Clinically, this kind of patients may complain of dryness of the mouth, difculties in chewing and swal-
lowing� seere periodontal disease or multiple caries� but usually they ollow an asymptomatic course. Saliary
gland aplasia can be diagnosed with a large ariety o imaging techniues� which include computer tomography(CT)� magnetic resonance imaging (M)� ultrasonography (S)� sialography� or scintigraphy. In this paper we
report a case o a patient reerred to our department with a long term and progressie growing neck mass� who has
an unilateral submandibular gland aplasia associated to an ipsilateral hypertrophy o the sublingual gland.
Key words: Submandibular gland aplasia, sublingual gland hypertrophy, neck mass.
errera-Calo G� García-Montesinos-Perea B� Saiz-Bustillo � Gallo-
Terán J� Lastra-García-Barón P. nilateral submandibular gland aplasia
with ipsilateral sublingual gland hypertrophy presenting as a neck mass.
Med Oral Patol Oral Cir Bucal . 2011 Jul 1;16 (4):e537-40.http://www.medicinaoral.com/medoralree01/16i4/medoral16i4p537.pd
Article Number: 16895 http://www.medicinaoral.com/
© Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946
eMail: [email protected]
Indexed in:Science Citation Inde Epanded
Journal Citation eports
Inde Medicus� MELINE� PubMed
Scopus� Embase and Emcare
Indice Mdico Español
doi:10.4317/medoral.16.e537
http://dx.doi.org/doi:10.4317/medoral.16.e537

8/6/2019 Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia
http://slidepdf.com/reader/full/ref-6-herrera-2011-unilateral-sub-mandibular-gland-aplasia 2/4
Med Oral Patol Oral Cir Bucal. 2011 Jul 1;16 (4):e537-40. Submandi bular gland aplasia with subling ual gland hyper trophy
e538
IntroductionMajor saliary gland agenesis is a ery uncommon
disorder. Since the rst case described in 1885, about
40 cases hae been reported in the literature. Most o
them were a congenital absence o all major saliary
glands. On the other hand� unilateral submandibular
gland aplasia is an etremely rare disorder. ccordingto our reiew� only 14 cases hae been described. Most
of them were incidental ndings because of the lack of
symptoms. In this study we report a case o an unilat-
eral submandibular gland aplasia with ipsilateral hyper-
trophy o the sublingual gland in a patient complaining
or a neck mass.
Case Report 26-year-old woman without any releant past medi-
cal or surgical history was reerred to our department
because o a long term submandibular swelling with
progressie growth. The patient didn’t complain about
any symptomatology, apart from a signicant anxiety
produced by the increasing size o the mass and the ig-
norance o her pathology.
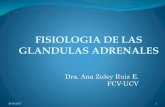
Inspection showed an asymmetry in the submandibular
region� due to a sot tissue enlargement at the right side
(Fig. 1), as well as some ipsilateral oor of the mouth
eleation. Etraoral palpation was unremarkable� butintraorally there was a lobulated painless and mobile
soft mass of about 2 centimetres in the right oor of
the mouth. Oral mucosa had no alterations. The rest o
oropharyngeal and cerical eamination was normal.
Fig. 1. Sot tissue enlargement in the right submandibular area.
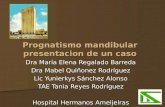
Fig. 2. ltrasonography o the right sublingual space (coronal cut).
Sublingual gland hypertrophy.
Fig. 3. T2-weightened images o magnetic resonance
(coronal cuts) � ight submandibular gland ab-
sence. B� ight sublingual gland hypertrophy.
B

8/6/2019 Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia
http://slidepdf.com/reader/full/ref-6-herrera-2011-unilateral-sub-mandibular-gland-aplasia 3/4
Med Oral Patol Oral Cir Bucal. 2011 Jul 1;16 (4):e537-40. Submandi bular gland aplasia with subling ual gland hyper trophy
e539
Neck S showed a slightly hyperechogenic homogene-
ous solid mass with smooth margins� located in the right
sublingual space (Fig. 2). No calcications or areas of
necrosis were noted. The right submandibular gland
could not be identied. No anomalies were observed in
the remaining major saliary glands� and cerical aden-
opathies were absent. These ndings were compatiblewith a hypertrophied right sublingual gland in associa-
tion with the absence o the ipsilateral submandibular
gland.
Our study was completed with M. ial and coronal
T1 and T2-weighted images showed absence o the right
submandibular gland and an enlarged right sublingual
gland� with the same signal characteristics as obsered
in the contralateral sublingual gland. ight sublingual
gland measured 22’38 12’47 millimetres� while the let
one measured 16’39 7’27 millimetres. Both parotid
glands and the let submandibular gland were normal�
as well as the rest o the study (Fig. 3).
DiscussionSaliary glands arise seuentially between the ourth
and the eighth week o etal deelopment as solid epi-
thelial buds rom primary oral caity� which grow and
etend into the underlying mesenchymal tissue as a sol-
id core o cells� which then undergoes etensie branch-
ing and eentually deelops lumina. Parotid glands ap-
pear during de ourth week o gestation� submandibular
glands during the sith� and sublingual glands during
the ninth (1).
The etiology o major saliary glands aplasia is still un-
known. This entity can accompany other deelopmental
anomalies� such as Treacher-Collins syndrome� hemia-
cial microsomia� clet palate or absence o the lacrimal
puncta (2�3). These abnormalities suggest that this en-3). These abnormalities suggest that this en-
tity may be associated with ectodermal deects o the
rst and second branchial arches and may be the result
of some disturbing inuence in early fetal development
(4). oweer congenital unilateral absence o the sub-
mandibular gland is not associated with other deelop-
ing anomalies� as well as our patient� which suggests
that this is an isolated phenomenon deried rom other
uniue deect o etal deelopment (5).
Clinical maniestations o the patients with saliarygland aplasia can ary depending on the number o
glands affected, their contribution in the salivary ow
production� and the presence o compensatory hypertro-
phy o the other glands. Some o them may be asympto-
matic� while others may present dryness o the mouth�
chewing and swallowing difculties or an increased in-
cidence o dental caries. This act is thought to be due
to reduction o the protectie eect o salia within the
oral caity (2).
Most o the patients with unilateral submandibular
gland aplasia reported in the literature had no symp-
toms related to the saliary gland absence� as well as
our case. Only two cases had dry lips and mouth� di-
culties with chewing solid oods and changes in taste
(6�7). A neck mass appearance as rst manifestation
has been only described three times� in two o them be-
cause o a compensatory gland hypertrophy (8)� and in
the other case because o a pleomorphic adenoma o thecontralateral submandibular gland (9). nilateral sub-
mandibular masses can be attributed to a high number
o pathologies with seeral origins. In the case described
by Shipchandler y Lorenz (8) the patient had a history o
suamous cell carcinoma o the tongue ipsilateral to the
mass, so the differential diagnosis was rst established
with a metastatic lymphadenopathy. Our patient had no
history o oral caity carcinoma. Other diagnostic pos-
sibilities considered were chronic sialadenitis, inam-
matory lymphadenopathy� saliary gland tumor and
lipoma.
Saliary gland aplasia can be diagnosed with a ariety
o imaging techniues� which include CT� M imaging�
S� sialography or scintigraphy (2�3�10). S is an ideal
tool for initial assessment of lesions in the supercial
parotid and submandibular gland. oweer� lesions in
the sublingual gland� located deeper and with a higher
percentage o malignant tumors� should be ealuated
by M imaging (11). CT cannot successully dieren-
tiate the sublingual gland rom the neighbouring mus-
cles. oweer� the ability o M imaging to dierenti-
ate the sublingual gland rom the surrounding tissues
acilitates the dierential diagnosis o the lesions in
this space. The sublingual gland has intermediate T1-
weighted signal intensity� lower than the at and higher than the muscle. On T2-weighted images the sublingual
gland remains hyperintense to muscle. Scintigraphy has
been described in some cases in the literature (2�3�12)�
but although this is a good method or determining the
unctional actiity o the saliary glands� it doesn’t de-
ne their anatomy (9). This technique may be useful for
discarding malignant origin in patients with personal
history of malignant tumors, as well as the ne needle
aspiration biopsy (FN) (8). Sialography by cannulat-
ing Wharton’s duct has also been used or submandibu-
lar gland agenesis conrmation (5). In our patient, US
was used as rst imaging technique showing the rightsubmandibular gland aplasia; this ecographyc ndings
were conrmed by MR imaging, which demonstrated
the ipsilateral sublingual gland hypertrophy.
The assessment o the patient and his amily is es-
sential� and ollow up seems to be worthwhile. Some
authors think that transoral sublingual gland ecision
should be considered in cases where the swelling were
aesthetically bothersome. In our case� the diagnosis and
the eclusion o other pathologies was enough or the
patient� who reused any therapy.
In conclusion� unilateral submandibular gland aplasia

8/6/2019 Ref 6 Herrera-2011-Unilateral Sub Mandibular Gland Aplasia
http://slidepdf.com/reader/full/ref-6-herrera-2011-unilateral-sub-mandibular-gland-aplasia 4/4
Med Oral Patol Oral Cir Bucal. 2011 Jul 1;16 (4):e537-40. Submandi bular gland aplasia with subling ual gland hyper trophy
e540
is an etremely rare disorder� and its real incidence is
probably unknown. Careul ealuation o the patients
who complain o erostomy� chewing and swallowing
difculties, severe periodontal disease and a neck mass,
may lead to the detection o new cases o this entity.
S and M imaging are adeuate techniues or this
patient’s study.
References1. Johns ME. The saliary glands: anatomy and embryology. Oto-
laryngol Clin North m. 1977;10:261-71.
2. Mconald FG� Mantas J� McEwen CG� Ferguson MM. Saliary
gland aplasia: an ectodermal disorder? J Oral Pathol. 1986;15:115-7.
3. igashino � orii T� Ohkusa Y� Ohkuma � Ino C� Nakazawa
M� et al. Congenital absence o lacrimal puncta and o all major sa-
liary glands: case report and literature reiew. Clin Pediatr (Phila).
1987;26:366-8.
4. Kubo S� be K� reshino T� Oka M. plasia o the submandibular
gland. case report. J Craniomailloac Surg. 1990;18:119-21.
5. oh JL. nilateral submandibular gland aplasia: an isolated phe-
nomenon o early etal deelopment. Otolaryngol ead Neck Surg.
2006;135:332-4.6. Yilmaz M� Karaman E� Isildak � Ener O� Kilic F. Symptomatic
unilateral submandibular gland aplasia associated with ipsilateral su-
blingual gland hypertrophy. ysphagia. 2010;25:70-2.
7. Gallego L� Junuera L� Cuesta P� osado P. Symptomatic uni-
lateral submandibular gland aplasia. Br J Oral Mailloac Surg.
2009;47:243.
8. Shipchandler TZ� Lorenz . nilateral submandibular gland
aplasia masuerading as cancer nodal metastasis. m J Otolaryngol.
2008;29:432-4.
9. García-Consuegra L� Gutirrez LJ� Castro JM� Granado JF. Con-
genital unilateral absence o the submandibular gland. J Oral Mai-
lloac Surg. 1999;57:344-6.
10. Yoshiura K� Yamada M� Yamada N. emonstration o congeni-
tal absence o then major saliary glands by computed tomography.
entomailloac adiol. 1990;2:77-8.11. Lee YY� Wong KT� King � huja T. Imaging o saliary
gland tumours. Eur J adiol. 2008;66:419-36.
12. Sucupira MS� Weinreb JW� Camargo EE� Wagner N Jr. Sali-
ary gland imaging and radionuclide dacryocystography in agenesis
o saliary glands. rch Otolaryngol. 1983;109:197-8.
References with links to Crossref - DOI