Non-invasive diagnosis of intracranial aneurysmsNon-invasive diagnosis of intracranial aneurysms...
12
Diagnostic and Interventional Imaging (2014) 95, 1163—1174 CONTINUING EDUCATION PROGRAM: FOCUS. . . Non-invasive diagnosis of intracranial aneurysms C. Rodriguez-Régent a , M. Edjlali-Goujon a , D. Trystram a , G. Boulouis a , W. Ben Hassen a , S. Godon-Hardy a , F. Nataf c , A. Machet a,d , L. Legrand a , A. Ladoux a , C. Mellerio a , R. Souillard-Scemama a , C. Oppenheim a , J.-F. Meder a , O. Naggara a,∗,b a Department of Neuroradiology, INSERM UMR 894, Faculté de Médecine, Neurosciences and Psychiatry Centre, Sainte-Anne Hospital Centre, Université Paris Descartes Sorbonne Paris Cité, 1, rue Cabanis, 75014 Paris, France b Department of Pediatric Radiology, Faculté de Médecine, Necker Children’s Hospital, Université Paris Descartes, Sorbonne Paris Cité, rue de Sèvres, 75007 Paris, France c Department of Neurosurgery, INSERM UMR 894, Faculté de Médecine, Neurosciences and Psychiatry Centre, Sainte-Anne Hospital Centre, Université Paris Descartes Sorbonne Paris Cité, 1, rue Cabanis, 75014 Paris, France d Department of Radiology, Le Mans Hospital Center, France KEYWORDS Intracranial aneurysm; Hemorrhage; CT; MRI angiography Abstract Patients need to be examined for intracranial aneurysms if they have had a sub- arachnoid hemorrhage. The preferred technique in this situation is CT angiography. Screening can be done for familial forms or for elastic tissue disorders, for which the first line investi- gation is magnetic resonance angiography. These non-invasive methods have now taken over from conventional angiography that was reserved for the pretreatment phase. A good tech- nical knowledge of these imaging methods, their artifacts and misleading images enables reliable detection of intracranial aneurysms and for an accurate report to be returned to clinicians. © 2014 Éditions franc ¸aises de radiologie. Published by Elsevier Masson SAS. All rights reserved. ∗ Corresponding author. E-mail address: [email protected] (O. Naggara). http://dx.doi.org/10.1016/j.diii.2014.10.005 2211-5684/© 2014 Éditions franc ¸aises de radiologie. Published by Elsevier Masson SAS. All rights reserved.
Transcript of Non-invasive diagnosis of intracranial aneurysmsNon-invasive diagnosis of intracranial aneurysms...

Diagnostic and Interventional Imaging (2014) 95, 1163—1174
CONTINUING EDUCATION PROGRAM: FOCUS. . .
Non-invasive diagnosis of intracranialaneurysms
C. Rodriguez-Régenta, M. Edjlali-Goujona,D. Trystrama, G. Boulouisa, W. Ben Hassena,S. Godon-Hardya, F. Natafc, A. Macheta,d,L. Legranda, A. Ladouxa, C. Mellerioa,R. Souillard-Scemamaa, C. Oppenheima,J.-F. Medera, O. Naggaraa,∗,b
a Department of Neuroradiology, INSERM UMR 894, Faculté de Médecine, Neurosciences andPsychiatry Centre, Sainte-Anne Hospital Centre, Université Paris Descartes Sorbonne ParisCité, 1, rue Cabanis, 75014 Paris, Franceb Department of Pediatric Radiology, Faculté de Médecine, Necker Children’s Hospital,Université Paris Descartes, Sorbonne Paris Cité, rue de Sèvres, 75007 Paris, Francec Department of Neurosurgery, INSERM UMR 894, Faculté de Médecine, Neurosciences andPsychiatry Centre, Sainte-Anne Hospital Centre, Université Paris Descartes Sorbonne ParisCité, 1, rue Cabanis, 75014 Paris, Franced Department of Radiology, Le Mans Hospital Center, France
KEYWORDSIntracranialaneurysm;Hemorrhage;CT;MRI angiography
Abstract Patients need to be examined for intracranial aneurysms if they have had a sub-arachnoid hemorrhage. The preferred technique in this situation is CT angiography. Screeningcan be done for familial forms or for elastic tissue disorders, for which the first line investi-gation is magnetic resonance angiography. These non-invasive methods have now taken overfrom conventional angiography that was reserved for the pretreatment phase. A good tech-nical knowledge of these imaging methods, their artifacts and misleading images enablesreliable detection of intracranial aneurysms and for an accurate report to be returned to
clinicians.© 2014 Éditions francaises de rad∗ Corresponding author.E-mail address: [email protected] (O. Naggara).
http://dx.doi.org/10.1016/j.diii.2014.10.0052211-5684/© 2014 Éditions francaises de radiologie. Published by Elsevie
iologie. Published by Elsevier Masson SAS. All rights reserved.
r Masson SAS. All rights reserved.

1
otsadftadtfi
G
P
Anlrd
bs
fpt[bilo
m•
•
Fscccp
164
Seventy-five per cent of spontaneous subarachnoid hem-rrhages (SAH) or cerebral-meningeal hemorrhages are dueo rupture of an intracranial aneurysm for which patientshould be examined on an urgent basis. A family history in
first-degree relative, or a risk factor such as elastic tissueisease or polycystic renal disease should prompt screeningor unruptured intracranial aneurysms. In all of these situa-ions it is important to know how to detect an intracranialneurysm, choose the best non-invasive imaging techniqueepending on the patient’s clinical state, understand theechnical settings for each modality and the diagnostic pit-alls to be avoided and finally to know which information ismportant to provide to the clinician in the report.
eneral information
athophysiology
n intracranial aneurysm is a local dilation of an intracra-ial artery. In the vast majority of cases it is an acquiredesion. Intracranial aneurysms are rare in children and veryare in the neonatal period [1]. The pathophysiology of their
evelopment remains extremely controversial.It has been suggested that genetic factors are involvedecause of the presence of familial forms and multipleites have been found [2]. Involvement of environmental
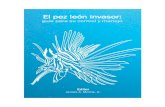
igure 1. Different forms of intracranial aneurysm. Aneurysms with aeen on catheterized angiography. a: left motor cortex saccular aneuralloso-marginal low flow aneurysms associated with an arterio-venous
erebral artery; e: dissecting left carotid artery aneurysm; f: post-traumavernous fistula (opacification of the cavernous sinus around the carotietrous sinus posteriorly).
C. Rodriguez-Régent et al.
actors such as hypertension, chronic alcoholism and theatient being an active smoker are well documented inhe development of intimal intracranial artery wall lesions3—5]. An intimal abnormality due to disturbance of locallood flow [6] occurring in genetically predisposed patientss believed to cause fragmentation of the internal elasticayer and the media, from which the aneurysm devel-ps.
In addition to ‘‘degenerative’’ saccular aneurysms, otherore rare forms of aneurysm also exist (Fig. 1):‘‘true’’ aneurysms with a wall:◦ non-dissecting fusiform aneurysms, which may be con-
genital or ‘‘degenerative’’, secondary to arterial walldisease (atheroma, hypertension),
◦ high flow rate aneurysms associated with arterio-venous malformations due to increased blood flow inthe afferent arteries;
pseudo-aneurysms which do not have a wall:◦ mycotic aneurysms due to a leukocyte infiltrate which
destroys the arterial wall and complicates 5% of casesof endocarditis: these aneurysms are fusiform or (morerarely) saccular, irregular in outline and in particularare located distally and spare the circle of Willis,
◦ dissecting aneurysms which are typically fusiform orfusiform-saccular and occur after intimal damage lead-ing to the formation of a secondary channel betweenthe limiting elastic interna and the media,
wall (a, b, c) and without a wall or pseudo-aneurysms (d, e, f),ysm; b: left multi cortex fusiform aneurysm; c: peri-callosal andmalformation; d: mycotic aneurysm of segment M2 of the middleatic aneurysm of the carotid siphon associated with direct carotidd siphon from the superior ophthalmic vein anteriorly and inferior

S
IrsasrartpecanOasitni
Non-invasive diagnosis of intracranial aneurysms
◦ traumatic aneurysms, as a result of injury from sud-den deceleration or a cranio-cerebral wound directlyinflicting lesions on the arterial wall. These are pseudo-aneurysmal sacs without a wall per se.
This review is restricted to ‘‘degenerative’’ saccularaneurysms.
Epidemiology
The prevalence of intracranial aneurysms varies dependingon whether the study is prospective or retrospective andon the study population. The prevalence ranges from 0.8to 4.6% in the general population, depending on the series,with a female predominance (sex-ratio 2.2—2.4) [7]. Riskfactors for intracranial aneurysm are age, being female, anactive smoking habit and hypertension [8,9]. Rare famil-ial forms are found: for a given patient, these forms aredefined by the presence of at least two first-degree rela-tives with intracranial aneurysms. Screening is indicated inthese situations [2,10]. These aneurysms are not transmitted
on a mendelian basis and this reflects genetic hetero-geneity. Intracranial aneurysms are also more common inautosomal dominant polycystic renal disease and hereditaryconnective tissue disorders such as type IV Ehlers-Danlossyndrome, type I neurofibromatosis and fibromusculardysplasia [8].M
Ta
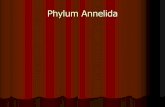
Figure 2. The most common locations for degenerative saccular aneuanterior communicating artery aneurysm; c: left carotid artery terminatiartery; e: aneurysm at the origin of the left postero-inferior cerebellar a
1165
ite
ntracranial aneurysms develop preferentially in the arte-ial part of the circle of Willis (70 to 90% depending on thetudies) (Fig. 2): 20 to 36% in the anterior communicatingrtery and anterior cerebral artery; 11 to 40% in the carotidiphon, end of the carotid artery and origin of the poste-ior communicating artery; 15 to 31% in the middle cerebralrtery and 10 to 30% are located in the cerebro-basilar arte-ial system (primarily at the end of the basilar artery and athe origin of the postero-inferior cerebellar artery). Multi-le aneurysms are present in 15 to 20% of cases [11,12]. It isssential with carotid siphon aneurysms to establish the spe-ific segment from which the aneurysm has developed. Someneurysms develop in the intra-cavernosal segments and doot carry a risk of subarachnoid hemorrhage if they rupture.n the other hand those which develop in segment C1 and C2re subarachnoid, as is the case for localized carotid caval,uperior pituitary, peri-ophthalmic, posterior communicat-ng and anterior choroid aneurysms) (Fig. 3). If it is suspectedhat an aneurysm may be extra-dural, a T2 weighted coro-al image may be useful as this shows the upper limit of thentra-cavernosal carotid artery (Fig. 4).
ethod of presentation
he feared method of presentation of intracranialneurysms is subarachnoid hemorrhage due to rupture of
rysms illustrated in real time MRA. a: overall MRA, caudal view; b:on aneurysm; d: aneurysm of the bifurcation of the middle cerebralrtery; f: aneurysm of the termination of the basal artery.

1166 C. Rodriguez-Régent et al.
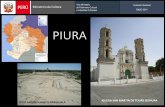
Figure 3. Carotid siphon aneurysms. a: oblique MRA view in real time of the right internal carotid artery. Terminal segment of theinternal carotid artery (ICA): segment C1 (1). Ophthalmic segment of the ICA: segment C2 (2). Clinoid segment of the ICA: segment C3 (3).Horizontal cavernous segment of the ICA: segment C4 (4). Ascending cavernous segment of the ICA: segment C5 (5). Segments 3,4 and 5are the cavernous ICA; b: location of carotid siphon aneurysms (A: cavernous aneurysm; B: carotid-caval aneurysm; C: superior hypophyseala municc
tha‘tnprio
ro
saa
Ftlst
neurysm; D: peri-ophthalmic aneurysm; E: carotid-posterior comommunicating artery. Shaded: cavernous sinus).
he aneurysmal sac. Headaches associated with meningealemorrhage are sudden in their onset, developing within
minute and occurring with no prodrome. The term‘thunderclap headaches’’ is used. These are severe fromhe outset and continuous and are often associated withausea and vomiting. Sudden onset headaches may be the
resenting feature of an aneurysm, which is not necessarilyuptured, in which case the term ‘‘sentinel headaches’’s used which describes a pre-rupture state with fissuringf the aneurysm. Circle of Willis imaging is thereforemico
igure 4. Superior hypophyseal artery aneurysm. MRA 3D TOF SS showhe junction of segments C2 and C3 (a). In a carotid siphon aneurysm thocated in C1 and C2. The T2 weighted coronal image (b) shows whetherinus towards segment C2, in the subarachnoid area. This shows that thehe cavernous sinus (distal dural ring or foramen of Kobayashi), shown b
ating artery aneurysm; F: anterior choroid aneurysm. PC: poster
ecommended for sudden onset headaches, even withoutvert SAH.
Cranial nerve paralysis or localizing focal neurologicaligns can be seen and are caused by the mass effect of
large aneurysm (classically a posterior communicatingrtery aneurysm compressing the third cranial nerve pair),
igration of an embolism from an aneurysmal thrombus orntra-parenchymal bleed and, more rarely, from late onseterebral ischemia as a result of vasospasm, the incidencef which peaks 4—12 days after rupture. The main manner
s an aneurysm of the left carotid siphon which has developed ate risk of subarachnoid hemorrhage is only present with aneurysms
a portion of the aneurysm has developed outside of the cavernous superior part of the aneurysm (arrow) is located above the roof ofy the dotted line and therefore located in the subarachnoid area.

cvajpqv
TiTd1i(rtSsinoa
amtdf
M
M3gsi•••
foraozvgt
aTod
Non-invasive diagnosis of intracranial aneurysms
in which intracranial aneurysms are discovered nowadays isas an incidental finding because of increased diffusion onimaging sections.
Indications for imaging
Thunderclap headaches are a formal indication for urgentcerebral imaging. Unenhanced cerebral CT is the most com-monly carried out investigation to exclude SAH and althoughthe sensitivity of cerebral CT is high in the acute phase, anormal cerebral CT does not obviate the need for a lum-bar puncture particularly if it is performed over 6 hoursafter symptoms have developed [13—15]. If MRI is acces-sible, FLAIR, T2* susceptibility weighted imaging (SWI) canbe used instead of unenhanced CT and is more sensitive todiagnose meningeal hemorrhage [16,17].
Screening may be offered in cases of autosomal domi-nant polycystic renal disease, hereditary.connective tissuedisorders (type IV Ehlers-Danlos syndrome, type I neu-rofibromatosis, fibromuscular dysplasia) or if at least twofirst-degree relatives have intracranial aneurysms [2,18].
Imaging methods
Conventional angiography
Conventional cerebral angiography offers excellent spa-tial resolution and provides a dynamic study of the entirecerebral vasculature. It is still the reference technique toidentify intracranial aneurysms. Using 3 dimensional acqui-sitions it provides a very accurate characterization of themorphology of the aneurysm, its shape, contours and regu-larity, measurement of sac size and particularly dimensionsof the neck of the aneurysm and the anatomy of the arteryinvolved and its neighboring branches. Conventional angiog-raphy, however, is an invasive investigation [19], which isless commonly accessible, expensive and involves irradiationto the patient and doctor. For this reason it is currently notperformed for a positive diagnosis of aneurysm but ratheris performed in order to plan treatment, or only in theinitial stage under general anesthesia before endovascularstenting. The large reduction in the number of conventionaldiagnostic angiographies performed has been due to thedevelopment of non-invasive CT and MR angiography tech-niques.
Cerebral CT angiography
Investigation techniqueCerebral CT angiography is a non-invasive technique, whichis very quick to perform, can be carried out on an urgentbasis and can be used to supplement unenhanced CT whichhas diagnosed subarachnoid hemorrhage. The iodine con-trast medium is injected via an automatic injector (40 to80 mL of contrast medium at 3 mL/second) and a region ofinterest is placed in an infrapetrous internal carotid artery.If the density at that point reaches the threshold value (100
HU), the image is acquired automatically.The image volume should cover the brain from theoccipital foramen to the vertex in order not to missaneurysms developing at the origin of the posterior inferior
bMsi
1167
erebellar arteries and distal pre-callosal aneurysms. Theolume examined is then reconstructed in thin sections inn axial plane. Three-dimensional maximum intensity pro-ection (MIP) or volume rendering (VR) reconstructions canroduce angiographic views. In order to optimize imageuality reconstructions can be centered on a single arterialessel.
he performance of CT angiography in detectingntracranial aneurysmshe sensitivity and specificity of cerebral CT angiography toiagnose an intracranial aneurysm are 92.8 to 100% and 83 to00% respectively [11,20—24]. Performance varies depend-ng on the equipment used and type of population studiedall-comers or patients with meningeal hemorrhage). Theisk of missing an aneurysm is between 5 and 10%, althoughhis sensitivity varies depending on the size of the aneurysm.ensitivity appears to be poorer in aneurysms under 3 mm inize (64 to 74.1%) [23,25] and also appears to vary depend-ng on the site of the aneurysm. Therefore the main falseegative results are for aneurysms in intra osseous, petrousr carotid siphon segment. Several studies have shown VRnalysis to be superior to MIP in these sites (Fig. 5).
CT angiography offers excellent detection sensitivity butppears to be more limited in specific planning for a treat-ent procedure. Detection of arterial branches arising from
he aneurysmal sac, neck or close to the aneurysm, theimensions of the sac and neck are obtained more reliablyrom conventional angiography [26,27].
agnetic resonance angiography (MRA)
ain MRA imaging techniques for the circle of WillisD TOF MRI angiography is based on a 3D T1 weighted echoradient compensated for flow to emphasize the vascularignal in relation to the stationary proton signal in surround-ng tissues. The image appearance depends on:
the RT of the image;the image tilt angle;the T1 weighted appearance of tissues located within thevolume investigated.
Short repetition time echo gradient images are per-ormed to saturate all of the protons bound in a planef the image section. The short repetition time reducesegrowth of maximal fixed spin longitudinal magnetizationnd as a result measurable transverse magnetization. Inther terms, the bound proteins result in a very low or evenero image and only protons contained in circulating bloodessels which are not pre-excited display maximum lon-itudinal magnetization resulting in measureable maximalransverse magnetization and a strong image appearance.
It is useful to use presaturation bands in order to counter-ct the signals from vessels proximal to the volume selected.his principle involves the technique of applying a seriesf successive impulses to prevent any regrowth of longitu-inal magnetization and therefore extinguishes the image
efore it penetrates a region of interest. For circle of WillisRA, two presaturation bands are positioned in the superioragittal sinus and torcula, thereby selectively excluding themage from veins.

1168 C. Rodriguez-Régent et al.
Figure 5. MIP and VR reconstructions of the CT angiogram MRA and 3D arteriography. Forty-two-year old male patient with sudden onsetheadache as a result of subarachnoid hemorrhage and intra-ventricular hemorrhage (a). The SAH is predominantly around the right carotidsiphon. CT angiography of the circle of Willis in which the MIP reconstruction (b) shows no aneurysm. The VR reconstruction (c) showsirregularity of the lateral wall of the right ICA with no saccular appearance. On real time 3 T MRA the VR reconstruction shows a saccularimage (e), which is poorly individualized on MIP reconstruction (d) and confirmed on the 3D angiography VR reconstruction with directinjection into the right ICA (f). This 3D image routinely proceeds any embolization therapy (g). In this case, apart from positioning coils int ause
wnsti
TAadsflsidatit
OMfaasfet(
s
itwo3isai
PAibitithi
swwaf
Q
he sac (dotted arrow), stent remodeling was required (arrows) bec
In order to reduce out-of-phase effects due to the coilshen embolized aneurysms are being monitored the ETeeds to be reduced to under 3 msec. This improves theensitivity of the circulating arterial network or recanaliza-ion of the aneurysmal sac, which appears as a flow hyperntensity.
he utility of 3D TOF with gadolinium enhancements the vascular appearance obtained at real time is gener-ted by flow effects themselves, it is easy to understand theifficulties which this technique experiences when studyingtructures with very turbulent flow (giant aneurysms) or slowow (stenoses). Intravoxel out-of-phase and circulating spinaturation effects cause drops in the signal, artefactuallyncreasing a degree of stenosis or leading to an incorrectiagnosis of partially thrombosed aneurysm. An injection of
half dose of gadolinium chelate can recover the signal inhese borderline cases by a T1 shortening effect. Then, themage is therefore not depending on flow effects but only onhe presence of gadolinium within the vessels (Figs. 6 and 7).
ptimizing the investigation volumeRI angiography must be adapted to the protocol required
or the patient: in the management of an acute phase CVAnd optimizing the 3D TOF sequence parameters can achieven image acquisition time of approximately 2 minutes. Increening from aneurysm the acquisition sequence can lastor up to 9 minutes in order to obtain multi-slab cov-rage from the postero-inferior cerebella arteries (PICA)
o the peri-callosal arteries with high spatial resolutionFigs. 8 and 9) [28].Increasing the image acquisition volume when circulatingpin gradually loses its image appearance, requires several
WdTo
of the wide neck and limited depth of the sac.
nterlinked image acquisition volumes to be used: this ishe principal of ‘‘multi-block’’ overlap or ‘‘multi-slabs’’ inhich in general 3 slabs are required to correctly cover theccipital foramen to the peri-callosal vessels [25] (Fig. 10). A0% slab coverage avoids a loss in vascular signal at thenterface between two slabs. If this overlap is inadequate aignal loss artifact at the slab junction known as a venetianrtifact (with reference to the venetian stores) may hindernterpretation (Fig. 8).
ost-treatmentngiographic reconstructions are obtained by selecting
nformation in the volume containing the most intense imageefore summing these (MIP software). Ideally the analysiss performed axis-by-axis after separating out and isolatinghe different arterial vessels in the circle of Willis. Wherevert possible, this axis-by-axis reconstruction should endeavoro separate out and exclude the subcutaneous and orbitalyperintense fat and then isolate and analyze the vesselsndividually [29].
One of the pitfalls of this image is its sensitivity tohort T1 weighted environments (blood, fat, post-pituitary),hich appear hyper intense on a TOF view and they interfereith the analysis (false vascular images). Vessel by vesselnalysis and using the basic sections can overcome this pit-all.
uality criteria for MRA
hen an MRA 3D TOF report for the circle of Willis is pro-uced, it is simple to provide an assessment of MRA quality.he visualized arteries are a good quality criterion in termsf spatial definition: seeing an ophthalmic artery or anterior

Non-invasive diagnosis of intracranial aneurysms 1169
Figure 6. Defective visualization of the aneurysmal sac in real time MRA. Seventy-seven-year old female patient with a symptomaticsaccular aneurysm in segment P1 of the left posterior cerebral artery. Note the absence of homogeneous hyperintensity in the aneurysmalsac on the unenhanced real time MRA sections (a), which may suggest partial thrombosis. Heterogeneous appearance of the sac on FLAIR
e sacn of
tefista
TbMewatto
imaging (b). On the unenhanced CT angiography sections (c), thaneurysmal sac: angiographic confirmation by selective opacificatio
choroid artery indicates that the examination can be usedto study structures between 0.5 and 1 mm in size.
The first volume section must pass beneath the occipitalforamen and visualize the vertebral arteries as they passthrough the dura mater. The final section is located abovethe arterial bend in the corpus callosum (Fig. 10).
Diagnostic performance with 3D TOF MRAThe sensitivity and specificity of 3D TOF MRA to identify anintracranial aneurysm over 3 mm in size are 87 to 100% and86 to 100% respectively [30]. The results are better with3 Tesla MRI than with 1.5 Tesla MRI because of greater spa-tial resolution. At 3 Tesla, the sensitivity and specificity todetect aneurysms under 5 mm in size are 98 and 94% respec-tively [28].
Apart from a positive diagnosis of aneurysm, MRA shouldbe used to investigate for irregular scalloped, ‘‘pustular’’
appearances of the wall suggestive of fissure or rupture. Theartery or arteries with malformations need to be describedtogether with the appearance of the neck (wider ornarrower), shape of the aneurysm (base of origin wideri3mt
is fully filled, excluding the possibility of partially thrombosedthe left vertebral artery (d).
han depth: poor candidate for embolization) and the pres-nce or absence of an artery arising from the sac [31]. Anal key factor to investigate is whether the aneurysm isingle or multiple (20% of cases) beginning with an examina-ion of the equivalent contralateral arterial segment (mirrorneurysm).
he specific case of monitoring aneurysms treatedy remobilizationRA has a very important role to play in monitoringmbolized aneurysms and provides excellent correlationith angiographic results to identify recanalization of theneurysmal sac [32—35]. It is the recommended investiga-ion to monitor aneurysms treated by embolization [36]. Theechnical settings for the imaging need to be adjusted inrder to minimize artifacts due to the presence of plat-
num coils (shortening the echo time with an ET of undermsec). Some groups propose routine gadolinium enhance-ent to increase the sensitivity to identify recanalization of
he aneurysm [37].

1170 C. Rodriguez-Régent et al.
Figure 7. Improved visualization of the aneurysmal sac on real time MRA with gadolinium enhancement. Seventy-two-year old malepatient with a fusiform basilar artery aneurysm presenting with lower limb paresis, dysarthria and swallowing difficulties. Heterogeneousappearance of the sac on FLAIR imaging (a). Note the absence of a homogeneous hyper intensity in the aneurysmal sac on the unenhancedreal time MRA sections (b), which may suggest partial thrombosis. After enhancement with a half dose of gadolinium chelate (c) the sac isfully filled excluding the possibility of a partially thrombosed aneurysmal sac. The outlines of the aneurysm together with its morphologyand dimensions are difficult to assess on MIP reconstructions (d); this information becomes available after enhancement (e).
Figure 8. Positioning of a real time MRA image volume for the circle of Willis. Correct position (a) and incorrect position (b). Theinvestigation field should include caudally, the origin of the inferior cerebella arteries (lower arrows), and cranially, the branches of thedivision of the peri-callosal arteries (upper arrows), outside of the imaging field. This coverage requires the use of several slabs which needto be 30% overlapped; if overlapping is insufficient, a band of signal loss (dotted arrows in b) is seen at the intersection of the slabs andmay create an artefactual stenosis.

Non-invasive diagnosis of intracranial aneurysms 1171
Figure 9. MRA coverage defect. Subarachnoid hemorrhage predominantly in the posterior fossa. This is attributed to rupture of a 3 mmaneurysm at the termination of the basilar artery shown on the global postero-anterior view (a) of the real time MRA and on the selectiveposterior anterior view of the basilar artery (dotted arrow) (b). On catheterized angiography, selective opacification of the left vertebralartery (c) confirms the presence of the aneurysm (dotted arrow) and
(continuous arrow), not seen on MRA as it is outside of the field of vision
Figure 10. Positioning slabs for a real time MRA landmarkingimage in the sagittal plane. For investigational headache and anetiological assessment of the subarachnoid hemorrhage, the fieldof vision must include caudally, the origin of the inferior cerebellaarteries. The inferior slab (blue) should be positioned below theoccipital foramen. Cranially the MRA should include the dividingbranches of the peri-callosal arteries. The upper slab (green) shouldbe positioned above the bend of the corpus callosum. Note the over-lap between the different slabs involving at least a third of theirheight.
C
ShiftaicpoTaoTsloti
particularly reveals an 8 mm aneurysm at the origin of the PICA.
onclusion
ubarachnoid hemorrhage, thunderclap headaches, and aistory of an intracranial aneurysm in a first-degree fam-ly member are indications for 3D TOF MRA to investigateor an aneurysm. Whilst conventional angiography remainshe reference method, 3D TOF MRA at 1.5 Tesla provides
sensitivity of over 90% for aneurysms over 3 mm in sizen a non-invasive manner without as complicated a techni-al procedure. Joint examination of 3D maximum intensityrojection (MIP) reconstructions and unprocessed sectionsffers a sensitivity of over 90% and a specificity of 100% [31].he volume rendering (VR) 3D TOF reconstruction techniqueppears to offer better detection and improved assessmentf intracranial aneurysms plan MIP reconstructions [38].here does not appear to be a significant difference inensitivity between CT angiography and MRA [39]. Three mil-imeters appears to be a cut off below which the sensitivityf 1.5 Tesla MRA falls rapidly regardless of the reconstructionechnique used. Diagnostic performance is better at 3 Tesla,ncluding aneurysms under 5 mm in size.
TAKE-HOME MESSAGES
• MRA and CT angiography are taking over from digitalangiography to detect aneurysms, the latter beingreserved for the treatment stage for managing
intracranial aneurysms.
1172 C. Rodriguez-Régent et al.
• CT angiography is performed in the acute phase ofsubarachnoid hemorrhage after unenhanced imageacquisition because of the speed with which it canbe performed.
• MRA is reserved more for screening for unrupturedaneurysms in patients with a first-degree familyhistory of intracranial aneurysm or risk factor(connective tissue disease).
• 3Tesla MRA is more sensitive than 1.5 Tesla MRA in thedetection of intracranial aneurysms.
• Following embolization therapy, aneurysms may bemonitored by 3D TOF MRA. Some groups recommendgadolinium enhancement.
• The report should contain the following information:whether the wall is regular or irregular in appearance,the artery or arteries with malformations, theappearance of the neck (broad or narrow) the shape ofthe aneurysm (saccular or fusiform), its dimensions,the presence of an artery arising from the sac and
C
Q
1
2
3
F
4
5
A
QcQbpin the field of vision and are usually very clearly seen.
F
whether the aneurysm(s) is/are single or multiple.
linical case
uestions
. What do you think about this MRA (Fig. 11), performedfor sudden onset headache?1 — it is a real time MRA2 — there is no aneurysm in the anterior circulation3 — coverage is correct4 — coverage is incorrect
. The field of vision of a circle of Willis MRA:1 — changes with the indication2 — is from the protuberance to the corpus callosum3 — can be increased by volume addition4 — includes branches of the external carotid artery
. What do you conclude from this MRA (Fig. 12):
1 — artifact2 — cavernous sinus aneurysm3 — peri-ophthalmic aneurysmQae
igure 12. MRA.
igure 11. Imaging for sudden onset headache.
4 — posterior communicating aneurysm. The sensitivity of MRA to diagnose aneurysm
1 — is 90%2 — is 70% of the lesions less than 3 mm in size3 — increases with reconstruction artery by artery4 — increases the reconstruction artery by artery in VR
compared to MIP. What are the indications for gadolinium enhancement on
a TOF MRA?1 — investigation for angiitis2 — giant aneurysm3 — arterial obstruction4 — basal meningioma
nswers
1: 1, 2, 4. Defective cranial coverage that may miss a peri-allosal aneurysm (seen on Fig. 13).2: 1, 3, 4. Field of vision beneath the occipital foramen toelow the bend of the corpus callosum. The superficial tem-oral branches of the external carotid arteries are included
3: 1. The substances on short T1 imaging suchs fat, a hematoma (methemoglobin), with gadoliniumnhancement, produce a strong image, which is difficult

Non-invasive diagnosis of intracranial aneurysms
[
[
[
[
[
[
[
[
[
[
[
[
[
[
phy. AJNR Am J Neuroradiol 2007;28:60—7.
Figure 13. Same patient as Fig. 11.
to saturate. The post-MIP processing software cannot dis-tinguish this appearance from an appearance of circulatingblood and shows it on the angiography reconstructions hin-dering examination of the circle of Willis or leading toincorrect interpretations. In this case the H1 hyperintensityof the anterior clinoid fat is seen (cross).Q4: 1, 2, 3, 4.Q5: 1, 2, 3, 4. In a meningioma of the base of the cra-nium enhancement can quantify stenosis due to a tumor,as a result of compression or invasion.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
References
[1] Krings T, Geibprasert S, terBrugge KG. Pathomechanismsand treatment of pediatric aneurysms. Childs Nerv Syst2010;26:1309—18.
[2] Brown Jr RD, Broderick JP. Unruptured intracranial aneurysms:epidemiology, natural history, management options, and famil-ial screening. Lancet Neurol 2014;13:393—404.
[3] Liaw N, Dolan Fox JM, Siddiqui AH, Meng H, Kolega J. Endothe-lial nitric oxide synthase and superoxide mediate hemodynamicinitiation of intracranial aneurysms. PLoS ONE 2014;9:e101721.
[4] Chalouhi N, Hoh BL, Hasan D. Review of cerebralaneurysm formation, growth, and rupture. Stroke 2013;44:3613—22.
[5] Bacigaluppi S, Piccinelli M, Antiga L, et al. Factors affectingformation and rupture of intracranial saccular aneurysms. Neu-rosurg Rev 2014;37:1—14.
[6] Gao L, Hoi Y, Swartz DD, Kolega J, Siddiqui A, Meng H. Nascentaneurysm formation at the basilar terminus induced by hemo-dynamics. Stroke 2008;39:2085—90.
[
1173
[7] Vernooij MW, Ikram MA, Tanghe HL, et al. Incidental find-ings on brain MRI in the general population. N Engl J Med2007;357:1821—8.
[8] Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence ofunruptured intracranial aneurysms, with emphasis on sex, age,comorbidity, country, and time period: a systematic review andmeta-analysis. Lancet Neurol 2011;10:626—36.
[9] Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk ofrupture of intracranial aneurysms: a systematic review. Stroke1998;29:251—6.
10] Kelly AG. Unruptured intracranial aneurysms: screeningand management. Continuum (Minneap Minn) 2014;20:387—98.
11] Pozzi-Mucelli F, Bruni S, Doddi M, Calgaro A, Braini M, CovaM. Detection of intracranial aneurysms with 64 channel multi-detector row computed tomography: comparison with digitalsubtraction angiography. Eur J Radiol 2007;64:15—26.
12] White PM, Teasdale EM, Wardlaw JM, Easton V. Intracranialaneurysms: CT angiography and MR angiography for detectionprospective blinded comparison in a large patient cohort. Radi-ology 2001;219:739—49.
13] Connolly Jr ES, Rabinstein AA, Carhuapoma JR, et al. Guidelinesfor the management of aneurysmal subarachnoid hemorrhage:a guideline for healthcare professionals from the Ameri-can Heart Association/american Stroke Association. Stroke2012;43:1711—37.
14] Backes D, Rinkel GJ, Kemperman H, Linn FH, Vergouwen MD.Time-dependent test characteristics of head computed tomo-graphy in patients suspected of nontraumatic subarachnoidhemorrhage. Stroke 2012;43:2115—9.
15] Edlow JA, Panagos PD, Godwin SA, Thomas TL, DeckerWW. Clinical policy: critical issues in the evaluation andmanagement of adult patients presenting to the emer-gency department with acute headache. Ann Emerg Med2008;52:407—36.
16] Verma RK, Kottke R, Andereggen L, et al. Detecting subarach-noid hemorrhage: comparison of combined FLAIR/SWI versusCT. Eur J Radiol 2013;82:1539—45.
17] Mohamed M, Heasly DC, Yagmurlu B, Yousem DM. Fluid-attenuated inversion recovery MR imaging and subarachnoidhemorrhage: not a panacea. AJNR Am J Neuroradiol2004;25:545—50.
18] Bor AS, Rinkel GJ, van Norden J, Wermer MJ. Long-term, serialscreening for intracranial aneurysms in individuals with a fam-ily history of aneurysmal subarachnoid haemorrhage: a cohortstudy. Lancet Neurol 2014;13:385—92.
19] Fifi JT, Meyers PM, Lavine SD, et al. Complications of mod-ern diagnostic cerebral angiography in an academic medicalcenter. J Vasc Interv Radiol 2009;20:442—7.
20] Papke K, Kuhl CK, Fruth M, et al. Intracranial aneurysms: roleof multidetector CT angiography in diagnosis and endovasculartherapy planning. Radiology 2007;244:532—40.
21] Taschner CA, Thines L, Lernout M, Lejeune JP, Leclerc X. Treat-ment decision in ruptured intracranial aneurysms: comparisonbetween multi-detector row CT angiography and digital sub-traction angiography. J Neuroradiol 2007;34:243—9.
22] Villablanca JP, Jahan R, Hooshi P, et al. Detection andcharacterization of very small cerebral aneurysms by using2D and 3D helical CT angiography. AJNR Am J Neuroradiol2002;23:1187—98.
23] Yoon DY, Lim KJ, Choi CS, Cho BM, Oh SM, Chang SK. Detectionand characterization of intracranial aneurysms with 16-channelmultidetector row CT angiography: a prospective comparisonof volume-rendered images and digital subtraction angiogra-
24] Westerlaan HE, van Dijk JM, Jansen-van der Weide MC,et al. Intracranial aneurysms in patients with subarachnoidhemorrhage: CT angiography as a primary examination tool

1
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
174
for diagnosis–systematic review and meta-analysis. Radiology2011;258:134—45.
25] Korogi Y, Takahashi M, Katada K, et al. Intracranial aneurysms:detection with three-dimensional CT angiography with vol-ume rendering — Comparison with conventional angiographicand surgical findings. Radiology 1999;211:497—506.
26] Anxionnat R, Bracard S, Ducrocq X, et al. Intracranialaneurysms: clinical value of 3D digital subtraction angiogra-phy in the therapeutic decision and endovascular treatment.Radiology 2001;218:799—808.
27] Sugahara T, Korogi Y, Nakashima K, Hamatake S, Honda S,Takahashi M. Comparison of 2D and 3D digital subtractionangiography in evaluation of intracranial aneurysms. AJNR AmJ Neuroradiol 2002;23:1545—52.
28] Li MH, Li YD, Gu BX, et al. Accurate diagnosis of small cere-bral aneurysms ≤ 5 mm in diameter with 3.0-T MR angiography.Radiology 2014;271:553—60.
29] Li H, Yan L, Li MH, et al. Evaluation of intracranial aneurysmswith high-resolution MR angiography using single-arteryhighlighting technique: correlation with digital subtractionangiography. Radiol Med 2013;118:1379—87.
30] Sailer AM, Wagemans BA, Nelemans PJ, de Graaf R, van ZwamWH. Diagnosing intracranial aneurysms with MR angiography:systematic review and meta-analysis. Stroke 2014;45:119—26.
31] Adams WM, Laitt RD, Jackson A. The role of MR angiographyin the pretreatment assessment of intracranial aneurysms: acomparative study. AJNR Am J Neuroradiol 2000;21:1618—28.
32] Shankar JJ, Lum C, Parikh N, dos Santos M. Long-termprospective follow-up of intracranial aneurysms treated withendovascular coiling using contrast-enhanced MR angiography.AJNR Am J Neuroradiol 2010;31:1211—5.
C. Rodriguez-Régent et al.
33] Ferre JC, Carsin-Nicol B, Morandi X, et al. Time-of-flight MRangiography at 3 T versus digital subtraction angiography in theimaging follow-up of 51 intracranial aneurysms treated withcoils. Eur J Radiol 2009;72:365—9.
34] Wallace RC, Karis JP, Partovi S, Fiorella D. Non-invasiveimaging of treated cerebral aneurysms, part I: MR angiogra-phic follow-up of coiled aneurysms. AJNR Am J Neuroradiol2007;28:1001—8.
35] Anzalone N, Scomazzoni F, Cirillo M, et al. Follow-up of coiledcerebral aneurysms at 3 T: comparison of 3D time-of-flight MRangiography and contrast-enhanced MR angiography. AJNR AmJ Neuroradiol 2008;29:1530—6.
36] Schaafsma JD, Koffijberg H, Buskens E, Velthuis BK, van derGraaf Y, Rinkel GJ. Cost-effectiveness of magnetic resonanceangiography versus intra-arterial digital subtraction angiogra-phy to follow-up patients with coiled intracranial aneurysms.Stroke 2010;41:1736—42.
37] Gauvrit JY, Leclerc X, Caron S, Taschner CA, Lejeune JP, PruvoJP. Intracranial aneurysms treated with Guglielmi detachablecoils: imaging follow-up with contrast-enhanced MR angiogra-phy. Stroke 2006;37:1033—7.
38] Mallouhi A, Felber S, Chemelli A, et al. Detection and char-acterization of intracranial aneurysms with MR angiography:comparison of volume-rendering and maximum-intensity-projection algorithms. AJR Am J Roentgenol 2003;180:55—64.
39] Numminen J, Tarkiainen A, Niemela M, Porras M, Hernes-
niemi J, Kangasniemi M. Detection of unruptured cerebralartery aneurysms by MRA at 3.0 tesla: comparison with mul-tislice helical computed tomographic angiography. Acta Radiol2011;52:670—4.