Nefropatia de celulas falciformes
23
Nefropatía De Células Falciformes Dr. Cristhian Mauricio Bueno Lara Especialista en Medicina Interna – Universidad Autónoma de Bucaramanga Fellow en Nefrología – Universidad del Valle
-
Upload
cristhian-bueno-lara -
Category
Health & Medicine
-
view
161 -
download
2
Transcript of Nefropatia de celulas falciformes

Nefropatía De Células Falciformes
Dr. Cristhian Mauricio Bueno LaraEspecialista en Medicina Interna – Universidad Autónoma de Bucaramanga
Fellow en Nefrología – Universidad del Valle

Contenido
• Conceptos básicos de anatomía renal (Diapositiva 2)
• Fisiopatología de la nefropatía de células falciformes (Diapositiva 3 –10)
• Epidemiología (Diapositiva 11)
• Manifestaciones clínicas (Diapositiva 12)
• Diagnóstico y detección temprana (Diapositiva 13 - 15)
• Tratamiento (Diapositiva 16 – 22)
• Pronóstico (Diapositiva 23)

Conceptos básicos fisiología renal
1. Comprenhensive clinical nephrology 4th edition 2010

Fisiopatología
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297
2. Comprenhensive clinical nephrology 4th edition 2010
Hipoxia relativa, acidosis e hiperosmolaridad

Fisiopatología
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297
2. Comprenhensive clinical nephrology 4th edition 2010

Fisiopatología
Hiperfiltración
2012
Elevada tasa de filtración glomerular en la línea
de base del estudio en infantes con media de
edad de
13.7 años
1. Courtney D. Thornburg, Beatrice A. Files, Zhaoyu Luo, Scott T. Miller, Ram Kalpatthi, Rathi Iyer, Phillip Seaman, Jeffrey
Lebensburger, Ofelia Alvarez,9 Bruce Thompson, Russell E. Ware, and Winfred C. Wang, for the BABY HUG Investigators. Impact of
hydroxyurea on clinical events in the BABY HUG trial. Blood. 2012;120(22):4304-4310

Fisiopatología
• Aumento de la filtración glomerular por la fase vasodilatadora de la NCF.
• Aumento de la secreción tubular de creatinina al filtrado.
• Aumento del gasto cardiaco.
• Desaparición de la hiperfiltración posterior a los 30 años.
Hiperfiltración
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297

Fisiopatología
• Aumento de la tasa de incidencia de albuminuria con la edad.
• Un 4% de los pacientes con anemia de células falciformes progresan a
síndrome nefrótico.
• Asociación entre infección por parvovirus B19 y síndrome nefrótico
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297
Albuminuria y proteinuria

Fisiopatología
1. Lynn Quek, Claire Sharpe, Neelanjana Dutt, Sue Height, Marlene Allman, Moji Awogbade,1David C Rees, Mark Zuckerman and Swee
Lay TheinAcute. Human parvovirus B19 infection and nephrotic syndrome in patients with sickle cell disease. British Journal of
Haematology, 149, 289–291
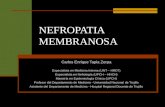
Acute human parvovirus B19 infect ion and nephrot ic syndrome
in pat ients w ith sickle cell disease
Human Parvovirus B19 (HPV B19) infection causessignificant
morbidity in patients with sickle cell disease (SCD) (Serjeant
et al, 1993, 2001; Smith-Whitley et al, 2004) and is a major
cause of transient red cell aplasia (TRCA) (Goldstein et al,
1987). It has also been previously suggested as a trigger of
nephrotic syndrome (NS) in patients with SCD (Wierenga
et al, 1995). The possible association between acute HPV B19
infection and NS was investigated in our cohort of SCD
patients. Information was gathered on (i) 37 individuals with
SCD of all ages admitted to King’s College Hospital (KCH)
with acute HPV B19 infection between November 2002 and
July 2008 and (ii) baseline HPV B19 status and indices of
proteinuria and renal function in a cohort of 317 adult SCD
patientswho attended thespecialist clinic between January and
December 2008.
The diagnosis of acute parvovirus B19 infection in aplastic
crisis was based on positive HPVB19 IgM, with or without
positive IgG, and past exposure to parvovirus infection based
on positive HPV B19 IgG. HPV B19 IgM and IgG antibodies
were detected by using antibody sandwich enzyme immuno-
assays (EIAs) according to manufacturers’ instructions. Red
cell aplasia wasdefined as a fall in haemoglobin concentration
to below steady-state levels of more than 30 g/l associated with
a very low reticulocyte count.
Of the37 individuals (median age8 years; range2–27 years)
with acute HPV B19 infection presenting with acute crisis and
TRCA, 29 were children below the age of 16 years, and eight
were patients over the age of 16 years. Thirty-two (25 below
16 yearsold and 7 over age16 years) of the37 patientshad the
HbSS genotype, two HbSC and three HbS b thalassaemia
genotypes. Three patients developed NS within 4 months of
acute HPV B19 infection and TRCA; Patient 1 at 17, Patient 2
at 26, and Patient 3 at 11 years of age at diagnosis.
Patient 1 had stable HbSC disease with a steady-state
haemoglobin level of 130–140 g/l and serum creatinine level
of between 70 and 80 l mol/l. In May 2004 he was admitted
with acute pain and dyspnoea. Investigations confirmed an
aplastic crisiswith ahaemoglobin level of 75 g/l and avery low
reticulocyte count of 5Æ3 · 1012 per litre (normal 50–
150 · 1012 per litre) associated with an acute parvovirus
Lynn Quek,1 Claire Sharpe,2,3 Neelanjana
Dutt,4 Sue Height,1 Marlene Allman,1
Moji Awogbade,1 David C Rees,1,3 Mark
Zuckerman5 and Swee Lay Thein1,3
1Department of Haematological Medicine,2Department of Renal Medicine, 3King’sCollege
London School of Medicine, Division of Gene and
Cell Based Therapy, 4Department of
Histopathology, and 5Department of Virology,
King’sCollege Hospital NHS Trust, Denmark
Hill, London, UK
Received 20 October 2009; accepted for
publication 28 November 2009
Correspondence: Swee L. Thein, King’s College
London School of Medicine, James Black
Centre, 125 Coldharbour Lane, London SE5
9NU, UK.
E-mail: [email protected]
Regrettably, Dr N Dutt died after submission of
the manuscript.
Summary
Acute Human Parvovirus B19 (HPV B19) infection is the major cause of
transient red cell aplasia (TRCA) and acute anaemia in patients with sickle
cell disease(SCD). Wereport threecasesof patientswho developed nephrotic
syndrome (NS) with chronic sequelae after initially presenting with HPV
B19-associated TRCA. There was no correlation between evidence of HPV
B19 infection and impaired renal function in our cohort of adult sickle cell
patients. This is consistent with a view that although NSis potentially a rare
complication of symptomatic acute HPV B19 infection, exposure to HPV
B19 is not associated with an increased risk of renal disease.
Keywords: parvovirus B19, nephrotic syndrome, sickle cell.
short report
First published online 7 January 2010
ª 2010 Blackwell Publishing Ltd, British Journal of Haematology, 149, 289–291 doi:10.1111/j.1365-2141.2009.08062.x
2010
Acute human parvovirus B19 infection and nephrotic syndrome
in patients with sickle cell disease
Human ParvovirusB19 (HPV B19) infection causessignificant
morbidity in patients with sickle cell disease (SCD) (Serjeant
et al, 1993, 2001; Smith-Whitley et al, 2004) and is a major
cause of transient red cell aplasia (TRCA) (Goldstein et al,
1987). It has also been previously suggested as a trigger of
nephrotic syndrome (NS) in patients with SCD (Wierenga
et al, 1995). The possible association between acute HPV B19
infection and NS was investigated in our cohort of SCD
patients. Information was gathered on (i) 37 individuals with
SCD of all ages admitted to King’s College Hospital (KCH)
with acute HPV B19 infection between November 2002 and
July 2008 and (ii) baseline HPV B19 status and indices of
proteinuria and renal function in a cohort of 317 adult SCD
patientswho attended thespecialist clinic between January and
December 2008.
The diagnosis of acute parvovirus B19 infection in aplastic
crisis was based on positive HPVB19 IgM, with or without
positive IgG, and past exposure to parvovirus infection based
on positive HPV B19 IgG. HPV B19 IgM and IgG antibodies
were detected by using antibody sandwich enzyme immuno-
assays (EIAs) according to manufacturers’ instructions. Red
cell aplasia wasdefined asa fall in haemoglobin concentration
to below steady-state levelsof morethan 30 g/l associated with
a very low reticulocyte count.
Of the37 individuals (median age8 years; range2–27 years)
with acuteHPV B19 infection presenting with acute crisisand
TRCA, 29 were children below the age of 16 years, and eight
were patients over the age of 16 years. Thirty-two (25 below
16 yearsold and 7over age16 years) of the37 patientshad the
HbSS genotype, two HbSC and three HbSb thalassaemia
genotypes. Three patients developed NS within 4 months of
acuteHPV B19 infection and TRCA; Patient 1 at 17, Patient 2
at 26, and Patient 3 at 11 years of age at diagnosis.
Patient 1 had stable HbSC disease with a steady-state
haemoglobin level of 130–140 g/l and serum creatinine level
of between 70 and 80 l mol/l. In May 2004 he was admitted
with acute pain and dyspnoea. Investigations confirmed an
aplastic crisiswith ahaemoglobin level of 75 g/l and avery low
reticulocyte count of 5Æ3 · 1012 per litre (normal 50–
150 · 1012 per litre) associated with an acute parvovirus
Lynn Quek,1Claire Sharpe,2,3Neelanjana
Dutt,4 Sue Height,1 Marlene Allman,1
Moji Awogbade,1 David C Rees,1,3 Mark
Zuckerman5 and Swee Lay Thein1,3
1Department of Haematological Medicine,2Department of Renal Medicine, 3King’sCollege
London School of Medicine, Division of Geneand
Cell Based Therapy, 4Department of
Histopathology, and 5Department of Virology,
King’sCollege Hospital NHSTrust, Denmark
Hill, London, UK
Received 20 October 2009; accepted for
publication 28 November 2009
Correspondence: Swee L. Thein, King’sCollege
London School of Medicine, James Black
Centre, 125 Coldharbour Lane, London SE5
9NU, UK.
E-mail: [email protected]
Regrettably, Dr N Dutt died after submission of
the manuscript.
Summary
Acute Human Parvovirus B19 (HPV B19) infection is the major cause of
transient red cell aplasia (TRCA) and acute anaemia in patients with sickle
cell disease(SCD). Wereport threecasesof patientswho developed nephrotic
syndrome (NS) with chronic sequelae after initially presenting with HPV
B19-associated TRCA. There was no correlation between evidence of HPV
B19 infection and impaired renal function in our cohort of adult sickle cell
patients. This isconsistent with a view that although NSispotentially a rare
complication of symptomatic acute HPV B19 infection, exposure to HPV
B19 is not associated with an increased risk of renal disease.
Keywords: parvovirus B19, nephrotic syndrome, sickle cell.
short report
First published online 7 January 2010
ª 2010 Blackwell Publishing Ltd, British Journal of Haematology, 149, 289–291 doi:10.1111/j.1365-2141.2009.08062.x
Microalbuminuria y proteinuria
No es posible establecer una relación directa entre el
síndrome nefrótico y parvovirus B19

Fisiopatología
• Hipostenuria en anemia de células falciformes.
• Alteraciones túbulos proximales y distales.
Anormalidades tubulares
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297
• Desde hematuria microscópica a macroscópica dolorosa.
• Excluir otras causas de hematuria.
Hematuria

Epidemiología
1. Claire C. Sharpe and Swee L. Thein. Sickle cell nephropathy – a practical British Journal of Haematology, 155, 287–297
2. Fabio D. Pereira, M.D.1, Isabel Sáenz, T.M.. Hemoglobinopatías en niños. Colombia Med 1996; 146- 149
3. Richard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
70.000 – 100.000
25%Nefropatía por Células
Falciformes 1% Población de raza negra de Tumaco
1996

Manifestaciones clínicas
1. ichard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
Hematuria
Nicturia
Poliuria
Lesión renal aguda (5 a 10%)
Enfermedad renal crónica
Síndrome nefrótico
Hipertensión

Diagnóstico
1. Geraldo Bezerra da Silva Junior, Alexandre Braga Libório, Elizabeth De Francesco Daher. New insights on pathophysiology, clinical
manifestations, diagnosis, and treatment of sickle cell nephropathy. Ann Hematol (2011) 90:1371–1379
Exámenes básicos
Uroanálisis
Depuración de creatinina de 24 horas
Ecuaciones para evaluar filtrado glomerular

Diagnóstico
Ecuaciones de filtrado glomerular
1. Nambirajan Sundaram, Michael Bennett, Jamie Wilhelm, Mi-Ok Kim, George Atweh, Prasad Devarajan, and Punam Malik. Biomarkers
for early detection of sickle nephropathy. Am. J. Hematol. 86:559–566, 2011
2011
116Pacientes con anemia de células
falciformes

Diagnóstico
1. E Voskaridou, E Terpos, S Michail, E Hantzi, A Anagnostopoulos, A Margeli, D Simirloglou, D Loukopoulos and I Papassotirio. Early
markers of renal dysfunction in patients with sickle cell/b-thalassemia. Kidney International (2006) 69, 2037–2042
Otros marcadores de nefropatía por células falciformes
Cistatina C
β2 - Microglobulina
2006
Cistatina C y β2 – Microglobulina sérica muestra una fuerte
relación con la creatinina y la edad del paciente.

Tratamiento
1. ichard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
Hidroxyurea y Nefropatía por células falciformes
2006
Sin TtoEnalapri
l+ Hidroxiurea
La combinación de terapias
debe ser efectuada en
pacientes con nefropatía por
células falciformes

Tratamiento
1. Sasongko TH, Nagalla S, Ballas SK. Angiotensin-converting enzyme (ACE) inhibitors for proteinuria and microalbuminuria in
people with sickle cell disease (Review)
Antagonistas SRAA y Nefropatía por células falciformes
Angiotensin-converting enzyme (ACE) inhibitors for
proteinuria and microalbuminuria in people with sickle cell
disease (Review)
Sasongko TH, Nagalla S, BallasSK
Thisisareprint of aCochranereview, prepared and maintained byTheCochraneCollaboration and published in TheCochraneLibrary
2013, Issue3
http://www.thecochranelibrary.com
Angiotensin-converting enzyme (ACE) inhibitors for proteinuria and microalbuminuria in people with sickle cell disease (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John W iley & Sons, Ltd.
2014
5 ensayos
clínicos
controlados
CaptoprilVs
Placebo
6 meses
seguimiento
pacientes con
proteinuria
Albuminuria
Proteinuria
No diferencias en estadísticamente
significativas en proteinuria y
albuminuria
Diferencias significativas en descenso
de cifras tensionales

Tratamiento
Management of Sickle Cell Disease Summary of the 2014 Evidence-Based Report by Expert Panel Members. JAMA. 2014;312(10):1033-
1048. doi:10.1001/jama.2014.10517
Antagonistas SRAA y Nefropatía por células falciformes
2014
Recomendación:
Para adultos con albuminuria sin otra causa aparente, iniciar
terapia con IECA (Nivel de evidencia 2B)

Tratamiento
1. ichard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
Transfusión de hemoderivados y Nefropatía por células falciformes
• Mantener la Hb < a 10 gr/dL y evitar aumentos de hematocrito mayores al
2% cada semana.
• El uso de agentes estimulantes de la eritropoyesis no se recomienda de
rutina en pacientes con nefropatía de células falciformes.

Tratamiento
1. ichard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
Terapia de reemplazo renal y Nefropatía por células falciformes
2002
Mortalidad en HDHR: 1.52 (IC= 1.27 – 1.82)
Mortalidad en TRHR: 1.1 (IC= 0.82 – 1.48)

Tratamiento
Management of Sickle Cell Disease Summary of the 2014 Evidence-Based Report by Expert Panel Members. JAMA. 2014;312(10):1033-
1048. doi:10.1001/jama.2014.10517
Antagonistas SRAA y Nefropatía por células falciformes
2014
Recomendación:
La terapia de reemplazo renal (Hemodiálisis, diálisis peritoneal y/o
trasplante renal) debe ser usada en pacientes con nefropatía por
células falciformes que la requieran (Nivel de evidencia 1C)

1. Jon I Scheinman. Sickle cell disease and the kidney.. doi:10.1038/ncpneph1008
Tra
tam
iento

Pronóstico
1. ichard Gargiulo, DO, Mauna Pandya, MD, Amber Seba, MD, Rami Y. Haddad, MD, Edgar V. Lerma, MD. Sickle cell nephropathy.
Disease-a-Month 60 (2014) 494–499
Terapia de reemplazo renal y Nefropatía por células falciformes
• Sobrevida = 4 años posterior a inicio de hemodiálisis.
• Riesgo de muerte es similar entre los pacientes con nefropatía y los
pacientes con enfermedad cerebrovascular.