Listas de Verificación de Seguridad Quirúrgica en Los Países en Desarrollo

of 5
Transcript of Listas de Verificación de Seguridad Quirúrgica en Los Países en Desarrollo
-
8/10/2019 Listas de Verificacin de Seguridad Quirrgica en Los Pases en Desarrollo
1/5
Review
Surgical safety checklists in developing countries
Sayinthen Vivekanant ham a , * , Rahul Prashanth Ravindran a, Kumaran Shanmugarajah b,Mahiben Maruthappu b, Joseph Shalhoub aa Imperial College School of Medicine, Imperial College London, London SW7 2AZ, UK b Harvard University, Cambridge, MA 01451, USA
a r t i c l e i n f o
Article history:Received 29 September 2013Accepted 24 October 2013Available online 13 November 2013
Keywords:SurgerySafetyChecklistsDeveloping countriesWorld Health Organization
a b s t r a c t
The World Health Organization Surgical Safety Checklist (WHO SSC) has demonstrated ef cacy indeveloped and developing countries alike. Recent increases in awareness of surgical morbidity indeveloping countries has placed greater emphasis on strategies to improve surgical safety in resource-limited settings. The implementation of surgical safety checklists in low-income countries has speci cbarriers related to resources and culture. Adapting and amending existing surgical safety checklists, aswell as considering factors unique to developing countries, may allow the potential of this simpleintervention to be fully harnessed in a wider setting.
This review will address the bene ts and challenges of implementation of surgical safety checklists indeveloping countries. Moreover, inspiration for the original checklist is revisited to identify areas thatwill be of particular bene t in a resource-poor setting. Potential future strategies to encourage theimplementation of checklists in these countries are also discussed.
2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
1. Introduction
The surgical mortality in developing countries is 10 times higherthan developed nations 1 and deaths attributed to anesthesia are1000-fold higher, 2,3 clearly demonstrating the need to improvesafety in this setting. By simply implementing checklists and pro-tocols from developed countries to developing countries we maynotbe harnessing their complete bene ts.This review will considerthe role of surgery in addressing the overall burden of disease in thedeveloping world and discuss the impact of the World Health Or-ganization Surgical Safety Checklist (WHO SSC) in this setting.Suggestions for appropriately adapting and expanding the WHOSSC for developing countries to improve the safety of surgeryglobally are also discussed. 4
2. Importance of surgery in developing countries
The recent WHO report Safe Surgery Saves Lives has helpedprioritize surgical care throughout the world. 5 Surgery has previ-ously been perceived to be a cost-ineffective intervention relative
to GDP in low-income countries.6
However, Gosselin et al. havemeasured the cost per Disability-Adjusted-Life-Year (DALY) in Si-erra Leone, which highlighted that the price per DALY averted was$32.78 through surgery, which compares favorably with non-surgical interventions. 7 Another study in Cambodia evaluated thecost of trauma surgery and this was also deemed to be cost-effective relative to other medical interventions. 8
Aside from cost being a barrier to the expansion of surgery indeveloping countries, it was also thought that surgery onlybene ted a small percentage of the population. This implied thatresources would be more effectively utilized on alternative man-agement strategies. Jamison et al. have countered this position;they have estimated that 11% of the global burden of disease can betreated by surgery, particularly by operating on those sufferingtrauma or cancer. 9
These ndings underpin the acknowledgment of the increasedbene t surgery can provide in developing countries. It is vital thatas increased surgical interventions are employed in these settings,safety standards are initiated and improved in parallel.
3. Importance of the WHO SSC in the developing world
Vast differences between developed and developing countries,for example in healthcare budgets, re ect differences in measuresneeded to ensure surgical safety. 9 In light of this, we believe theWHO SSCis even more critical in developing countries compared to
* Corresponding author. Tel.: 44 (0) 798101 5718.E-mail addresses: [email protected] (S. Vivekanantham),
[email protected] (R.P. Ravindran), [email protected] (K. Shanmugarajah), [email protected](M. Maruthappu), [email protected] (J. Shalhoub).
Contents lists available at ScienceDirect
International Journal of Surgery
j ou rna l homepage : www. jou rna l - surge ry.ne t
1743-9191/$ e see front matter 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ijsu.2013.10.016
International Journal of Surgery 12 (2014) 2 e 6
REVIEW
mailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]://www.sciencedirect.com/science/journal/17439191http://www.journal-surgery.net/http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://dx.doi.org/10.1016/j.ijsu.2013.10.016http://www.journal-surgery.net/http://www.sciencedirect.com/science/journal/17439191http://crossmark.crossref.org/dialog/?doi=10.1016/j.ijsu.2013.10.016&domain=pdfmailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected] -
8/10/2019 Listas de Verificacin de Seguridad Quirrgica en Los Pases en Desarrollo
2/5
developedcountries. For example,surgeons in rural areas may haveto perform a higher number of operations and operate in situationswhere they may not be specialists. 10 This maylead to simple checksbeing omitted because of the pressure of the workload, as well asunfamiliarity with the procedure performed. Checklists would beparticularly useful in such settings.
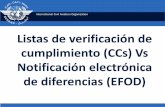
The WHO SSC was developed with the aim of routinely checkinginformation at three critical stages of surgery ( Fig. 1). Use of thisinitiative has been associated with reduced operative error andimproved outcomes. 4 In particular patient mortality fell from 1.5%to 0.8% following the implementation of this checklist. Importantly,this data was acquired from four high-income and four low-incomeor middle-income countries, as classi ed by the World Bank, 11
thereby demonstrating its applicability throughout the world. 4
Numerous other studies have looked into the implementation of the WHO SSC globally. 12e 14 In 2012, Borchard et al. performed asystematic review of the effectiveness of safety checklists in surgeryand encouragingly found that the relative risk of mortality fell to0.57 (95% CI:0.42 e 0.76) when checklists wereused. 14 Furthermore,
the relative risk of complications also fell after the implementationof the checklists (0.63 [95% CI: 0.58 e 0.67]). 14
Whilst the WHO SSC was trialed worldwide, evidence suggestsit is particularly effective in a resource-poor setting. Following theimplementation of the WHO SSC, the largest decrease in compli-cations (74.3%) was in low-income or middle-income countries. 4
Furthermore, in the same study, two of the four hospital sites inthe low-income and middle-income countries group had adecrease in surgical site infections and total complication rates,compared to only one of the four hospital sites in high-incomecountries. 4 These ndings highlight that the WHO SSC has thepotential for signi cant impact speci cally in the context of developing countries.
A possible explanation for these observations could be that anumber of safety measures outlined in the WHO SSC were alreadyused in developed countries prior to the formal introduction of thechecklist. For example, observations from high-income countriesfrom the initial WHO SSC study showed pulse oximetry was usedfor intra-operative monitoring in 99.0% of cases beforethe checklist
Fig. 1. Elements of the World Health Organization Surgical Safety Checklist. Reproduced with permission. 4
S. Vivekanantham et al. / International Journal of Surgery 12 (2014) 2 e 6 3
REVIEW
-
8/10/2019 Listas de Verificacin de Seguridad Quirrgica en Los Pases en Desarrollo
3/5
was introduced, compared to 86.0% in sites of low-income ormiddle-income countries. 4 In addition,prior to the implementationof the WHO SSC, intra-operative observers noted 63.9% of cases insites of high-income countries performed an oral con rmation of the patient s identity and surgical site prior to operation. However,this was only observed in 34.3% of cases in developing countries. 4
These studies have identi ed areas in which the WHO SSC mayhave a particular impact in developing countries.
While studies on the WHO SSC have demonstrated encouragingoutcomes, its usage remains po or, with checklist compliance hav-ing been reported as low as 12%. 14,15 Cultural differences may play arole in the reduced uptake of surgical safety checklists in devel-oping countries. In Thai culture, for example, it is against societalnorm to make marks on other people 16 so this may prevent themmarking the operative site. Moreover, people in Thailand onlyintroduce themselves when meeting initially, and are typically shyabout expressing their position thereafter. This may explain whyteam members were more reluctant to introduce themselves byname and role during the time-out period. 17 Furthermore, eco-nomic limitations may limit the full implementation of the check-list because of the requirement of certain equipment which maynot be affordable in the developing world. 18 In Thailand, surgicalsite marking and hair removal were typically not completed priorto checklist implementation. 17 A contributing factor could beshortage of materials; however, these items were then acquiredfollowing the implementation of a checklist, which perhaps servedto highlight their absence.
We have established that whilst the WHO SSC has some ef cacyin the developing world, there still remains scope to improve itsbene ts there. We now shift focus to concentrate on ways that thiscould potentially be done.
4. Developing checklists in resource-limited settings using past inspiration
Checklists from other industries contributed towards thedevelopment of the WHO SSC. 19 In order to adapt the WHO SSC tofurther bene t surgical safety in developing countries, it may beuseful to revisit the founding principles that initially inspired thecreation of the checklist, and see if further lessons may be gleaned.
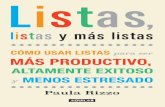
The high-pressure environment of surgery is found only in ahandful of other careers. Notably, Formula 1 (F1) racing and avia-tion both require high levels of teamwork, focus and performance,similar to that seen in an operating theater. This especially holdstrue in resource-limited theaters, often with a higher caseload. InF1, the pit stop requires the coordinated efforts of many teammembers to perform the necessary steps as ef ciently as possible(Fig. 2). In many ways this parallels the post-operative handoverprocess in surgery. In developing countries there is less staff to look
after patients and therefore correct and complete informationtransfer is critical. Considering this, variations or further criteriacould be introduced to the WHO SSC in developing countries tomaximize its bene t at the post-operative handover stage.
Catchpole et al. consulted the Ferrari F1 race director to identifysimilarities between surgical handover and racing safety. 20 Thisincluded, for example, the necessity of having a designated leader(in F1 this is the lollipop man and it was decided the anesthetistshould assume this role). 20 In developing countries, the role of theanesthetist is often assumed by nursing teams. This unclear de -nition as to who is responsible for completing the checklist maycontribute to lower usage in developing countries, due to confusionas to who should be responsible for delivering the checklist inresource-limited settings. Compliance could be improved through
creating tailored regional de nitions as to the speci c person who
is responsible for conducting the WHO SSC within the operatingtheaters in developing counties.
Meticulous training and practice is required for the ideal F1 pitstop; however, there is no structured training for the post-operativehandover, especially in developing countries. Catchpole et al. ac-counts for this, in part, by highlighting the low staff turnover in F1compared to constantly rotating doctors and nurses in the health-care world. Ensuring that staff work in the same roles as far aspossible, with minimal rotation between different positions, mighthelp further reduce complication rates in resource-limited settings.
Karl mentions several other factors that vary between surgeryand the aviation industry, beyond the use of checklists. 21 Forexample, in surgery there is an emphasis on documenting what isdone rather than actually focusing on doing it safely. Also in sur-
gery,people are expected to know how to deal with emergencies bymemory, whilst in aviation there is a quick reference handbook forall major emergencies that can be accessed for assistance. Utilizinga similar resource in developing countries to cover a range of emergency procedures might be a separate initiative that canimprove surgical safety globally. Finally, and importantly, below10,000 feet all airlines have sterile cockpit rules where there canbe no discussion apart from that which is relevant to the safety of the ight. 21 This is in contrast to surgery where there often isirrelevant discussion that is not policed, even during critical parts of a procedure. Incorporating sterile operating rules at key aspects of surgical procedures might help improve surgical safety in devel-oping and developed countries alike.
Although it is helpful to draw comparisons from other in-
dustries, ultimately surgical practice is unique. Therefore, whilst
Fig. 2. The different stages of the Formula 1 pit stop, where numbers denote the orderof the different actions. Reproduced with permission. 20
S. Vivekanantham et al. / International Journal of Surgery 12 (2014) 2 e 6 4
REVIEW
-
8/10/2019 Listas de Verificacin de Seguridad Quirrgica en Los Pases en Desarrollo
4/5
other industries standards of practice can be examined, weappreciate that not all lessons can be directly translated into sur-gery. We anticipate that these lessons will form the foundationupon which improvements to surgical practice can made, takinginto account the complexity and uniqueness of surgical patients.Surgical safety checklists have been shown to reduce errors;however, they have not completely eliminated them. This high-lights the ongoing importance of good clinical judgment and theappreciation of signi cant inter-patient variation by gaining expe-rience as a surgeon.
5. New directions for using checklists in resource-limitedsettings
While some studies have demonstrated a positive bene t of theWHO SSC there are ways in which checklists could be furtherdeveloped. Speci c checklists have been created to suit differentsurgical specialties, for example neurosurgery 22 and ophthal-mology. 23 At this time, it is unclear whether changes to content,structure, delivery and specialty-speci city of checklists could leadto further bene ts to patient safety and quality of treatment, withmore research in this area sure to provide the answer. With case-load variations between developed and developing countries interms of volume and types of procedures, use of checklists acrossdifferent specialties created in developed countries might need tobe further modi ed to ensure maximal bene t for use in resource-limited settings.
Although surgical research has been quick to embrace the po-tential of checklists, the adoption of checklists beyond the oper-ating room has been limited. 24 Checklists have been harnessedrecently in cardiac catheterization 25 and crisis situations. 26 Withfurther clinical situations trialing checklists in the developed world,it will become more readily apparent where bene t may be derivedthrough their implementation and give direction for further uses of checklists in developing settings.
In order to improve compliance in developing countries it may
be useful to adjust the WHO SSC, taking cultural variations intoaccount. Surgical practitioners of various ethnicities in differentcountries could be consulted to identify any speci c areas of thechecklist that might present a barrier to its uptake in regions withdifferent social norms. Amendments could then be made toaccommodate cultural variations.
The ef cacy of the WHO SSC has inspired the formation of various sister organizations that promote the use of medicalchecklists worldwide. Project Check is an umbrella organizationthat aims to act as a central source for all clinical checklists. Theorganization aims to make clinical checklists suitable for manydifferent situations globally, enhancing safety around the world. 15
Furthermore, the charity Lifebox was created to subsidize the costof purchasing pulse oximeters by hospitals in developing countries
as this may be a barrier to full implementation of the checklist inthese settings. 27 More recently, a study has demonstrated thatsuccessful implementation of the WHO SSC with provision of pulseoximeters in a resource-limited setting in Moldova resulted in areduction in overall post-operative complications from 21.5% to8.8%.28 Further initiatives to support the global implementation of checklists will help reduce surgical complications in developingsettings.
Checklist fatigue is when the overuse of checklists results inreduced overall compliance. The WHO SSC is designed to minimizethis by only including checks for common and preventable sourcesof error. 19 With the oc curr ence of checklist fatigue recognized inthe developed world, 29,30 measures to prevent this should beenforced in resource-limited settings. We believe this limitation is
less likely to occur if the previously outlined bene ts of using
checklists are stressed to those responsible for checklist compliancein developing countries. We also propose that following a reas-sessment of the components of the checklist, the checklist shouldbe tailored speci cally to various developing world settings, takinginto account cultural differences and local practices; only onechecklist should be implemented within a country or region.
6. Conclusions
It is estimated that at least half a million deaths per year wouldbe prevented worldwide if the WHO SSC was correctly imple-mented. 31 Any human system is prone to error; however, checklistsare proving to be an effective mechanism through which this can bereduced within surgery and beyond. We believe the bene ts fromthese measures will be of particular value in developing countries,where resources and surgical practice lag behind that of developedcountries.
Inspiration for developing safety checklists originated fromexamining protocols from other industries, where maintainingsafety is considered as important as achieving an outcome. Theseindustries provide ideas for further development of surgical safetychecklists, and there is an impetus to implement more ideas fromtheseother elds to improve the ef cacy of checklists in developingcountries. Whilst we acknowledge that checklists cannot replacegood clinical acumen, we feel that there is still scope for improvingsafety by increasing and adapting the usage of this tool in thedeveloping world.
Interventions to improve surgical safety through checklists ewhether pre-operatively, during surgery, post-operatively, or in acrisis setting e may also act as inspiration for other areas of med-icine. The direction and future application of these initiatives holdsmany possibilities and remains an exciting opportunity to furtherdrive down adverse outcomes within surgery, particularly indeveloping settings.
Con icts of interest Sayinthen Vivekanantham is founding Director of Global Med-
ical Education Trust (GMET), a recently established charity thataims to improve the quality of medical education and learningwithin healthcare in developing countries. Mahiben Maruthappu & Joseph Shalhoub are co-founding Directors and Kumaran Shan-mugarajah is the Secretaryof the World Surgical Association (WSA),a recently established non-pro t improving surgical care deliveryin resource-limited settings. They have no other con icts of interestto declare.
Funding None.
Ethical approval
None.
Author contributionSayinthen Vivekanantham e Extrapolation of initial concept,
drafting of the article, ideas for initiatives.Rahul Prashanth Ravindran e Drafting of the article, ideas for
initiatives.Kumaran Shanmugarajah e Review and editing of the article.Mahiben Maruthappu e Review and editing of the article. Joseph Shalhoub e Conception of idea, review and editing of the
article.
Acknowledgments
None.
S. Vivekanantham et al. / International Journal of Surgery 12 (2014) 2 e 6 5
REVIEW
-
8/10/2019 Listas de Verificacin de Seguridad Quirrgica en Los Pases en Desarrollo
5/5
References
1. Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the globalvolume of surgery: a modelling strategy based on available data. Lancet 2008; 372 (9633):139 e 44 .
2. Ouro-Bang na Maman AF, Tomta K, Ahouangbvi S, Chobli M. Deaths associatedwith anaesthesia in Togo, West Africa. Trop Doct 2005; 35 (4):220 e 2.
3. Li G, Warner M, Lang BH, Huang L, Sun LS. Epidemiology of anesthesia-related mortality in the United States, 1999 e 2005. Anesthesiology2009; 110 (4):759 e 65 .
4. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reducemorbidity and mortality in a global population. N Engl J Med 2009; 360 (5):491 e 9.
5. World Health Organisation. Safe surgery saves lives [cited 2013 12/04/13].Available from: http://who.int/patientsafety/safesurgery/en/index.html ; 2013.
6. Bickler SW, Spiegel D. Improving surgical care in low- and middle-incomecountries: a pivotal role for the World Health Organization. World J Surg 2010; 34 (3):386 e 90 .
7. Gosselin RA, Thind A, Bellardinelli A. Cost/DALY averted in a small hospital inSierra Leone: what is the relative contribution of different services? World J Surg 2006; 30 (4):505 e 11 .
8. Gosselin RA, Heitto M. Cost-effectiveness of a district trauma hospital in Bat-tambang, Cambodia. World J Surg 2008; 32 (11):2450 e 3.
9. Dean T, Jamison JGB, Measham Anthony R, et al. Disease control priorities indeveloping countries. 2nd ed.; 2006. p. 1 e 1448 .
10. Venkatesh R. Outcomes of high volume cataract surgeries in a developingcountry. Br J Ophthalmol 2005; 89 (9):1079 e 83 .
11. Bank W. Data & statistics: country classi cation . Available from: http://data.
worldbank.org/about/country-classi cations ; 2006.12. Bliss LA, Ross-Richardson CB, Sanzari LJ, et al. Thirty-day outcomes supportimplementation of a surgical safety checklist. ACS 2012; 215 (6):766 e 76 .
13. Fudickar A, Hrle K, Wiltfang J, Bein B. The effect of the WHO surgical safetychecklist on complication rate and communication. Dtsch rztebl Int 2012; 109 (42):695 e 701 .
14. Borchard A, Schwappach DLB, Barbir A, Bezzola P. A systematic review of theeffectiveness, compliance, and critical factors for implementation of safetychecklists in surgery. Ann Surg 2012; 256 (6):925 e 33 .
15. Spence J, Goodwin B, Enns C, Dean H. Student-observed surgical safetypractices across an urban regional health authority. BMJ Qual Saf 2011; 20 (7):580 e 6.
16. Kachru Y, Smith LE. Cultures, contexts, and world englishes, Routledge, 2008 .17. Kasatpibal N, Senaratana W, Chitreecheur J, Chotirosniramit N, Pakvipas P,
Junthasopeepun P. Implementation of the world health organization surgicalsafety checklist at a university hospital in Thailand. Surg Infect 2012; 13 (1):50 e 6.
18. Funk LM, Weiser TG, Berry WR, et al. Global operating theatre distribution andpulse oximetry supply: an estimation from reported data. Lancet 2010; 376 (9746):1055 e 61 .
19. Weiser TG, Haynes AB, Lashoher A, et al. Perspectives in quality: designing theWHO surgical safety checklist. Int J Qual Health Care 2010; 22 (5):365 e 70 .
20. Catchpole KR, De Leval MR, McEwan A, et al. Patient handover from surgery tointensive care: using Formula 1 pit-stop and aviation models to improve safetyand quality. Pediatr Anesth 2007; 17 (5):470 e 8.
21. Karl RC. Aviation. J Gastrointest Surg Off J Soc Surg Aliment Tract 2009; 13 (1):6 e 8.22. Zuckerman SL, Green CS, Carr KR, Dewan MC, Morone PJ, Mocco J. Neurosur-
gical checklists: a review. Neurosurg Focus 2012; 33 (5):E2 .23. Cavallini GM, Campi L, Maria M, Forlini M. Clinical risk management in eye
outpatient surgery: a new surgical safety checklist for cataract surgery andintravitreal anti-VEGF injection. Graefes Arch Clin Exp Ophthalmol 2012; 251 (3):889 e 94 .
24. Marjot T, Maruthappu M, Shalhoub J. Checklists for invasive procedures. N Engl J Med 2013; 368 (3):293 e 4.
25. Regueiro A, Price S, Haxby EJ. Minimizing risk in the cardiac catheterizationlaboratory. Rev Esp Cardiol (Engl Ed) 2013:1 e 4.
26. Arriaga AF, Bader AM, Wong JM, et al. Simulation-based trial of surgical-crisischecklists. N Engl J Med 2013; 368 (3):246 e 53 .
27. Merry A, Eichhorn J, Wilson I. Extending the WHO safe surgery saves lives
project through global oximetry. Anaesthesia 2009:1045 e 50 .28. Kwok AC, Funk LM, Baltaga R, et al. Implementation of the world health or-
ganization surgical safety checklist, including introduction of pulse oximetry,in a resource-limited setting. Ann Surg 2013; 257 (4):633 e 9.
29. Hales B, Terblanche M, Fowler R, Sibbald W. Development of medical check-lists for improved quality of patient care. Int J Qual Health Care 2007; 20 (1):22 e30 .
30. Hales BM, Pronovost PJ. The checklist d a tool for error management and per-formance improvement. J Crit Care 2006; 21 (3):231 e 5.
31. World Health Organisation. New scienti c evidence supports WHO ndings: asurgical safety checklist could save hundreds of thousands of lives [cited 2013 12/04/13]. Available from: http://who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.html ; 2013.
S. Vivekanantham et al. / International Journal of Surgery 12 (2014) 2 e 6 6
REVIEW
http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://who.int/patientsafety/safesurgery/en/index.htmlhttp://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://data.worldbank.org/about/country-classificationshttp://data.worldbank.org/about/country-classificationshttp://data.worldbank.org/about/country-classificationshttp://data.worldbank.org/about/country-classificationshttp://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref16http://refhub.elsevier.com/S1743-9191(13)01091-1/sref16http://refhub.elsevier.com/S1743-9191(13)01091-1/sref16http://refhub.elsevier.com/S1743-9191(13)01091-1/sref16http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.htmlhttp://who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.htmlhttp://who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.htmlhttp://who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.htmlhttp://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref30http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref29http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref28http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref27http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref26http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref25http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref24http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref23http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref22http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref21http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref20http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref19http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref18http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref17http://refhub.elsevier.com/S1743-9191(13)01091-1/sref16http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref15http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref14http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref13http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://refhub.elsevier.com/S1743-9191(13)01091-1/sref12http://data.worldbank.org/about/country-classificationshttp://data.worldbank.org/about/country-classificationshttp://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref10http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref9http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref8http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref7http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://refhub.elsevier.com/S1743-9191(13)01091-1/sref6http://who.int/patientsafety/safesurgery/en/index.htmlhttp://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref4http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref3http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref2http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1http://refhub.elsevier.com/S1743-9191(13)01091-1/sref1