
INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
9
INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS CPK (24 - 195 U/L); CKMB ( até 16 U/L); Creatine kinase-MB SI UNITS: 0±7 µg/L CONVENTIONAL UNITS: 0±7 ng/mL Troponina T e I; Troponin I: SI UNITS: 0 ±0.4 µg/L CONVENTIONAL UNITS: 0±0.4 ng/Ml Troponin T SI UNITS: 0±0.1 µg/L CONVENTIONAL UNITS: 0±0.1 ng/mL Mioglobinas. Myoglobin S Male: 19± 92 µg/L Female: 12±76 µg/L Troponina T Detectada de 3 a 12 horas após o IAM No sangue até 10 dias Níveis de 0,1 a 0,2 ng/ml Dosar admissão, 4, 8 e 16 horas Estudo de Peacock et al, com 266 pts, sensibilidade de 9,5% e especificidade de 99,2% na predição de eventos adversos. Troponina I Não é expressa em músculo esquelético hu mano durante o desenvolvimento fetal, após trauma ou durante regeneração da musculatura esquelética .É altamente específica para o miocárdio. No sangue de 7 a 10 dias após a necrose Estudo de Antman et al, com 1404 pts, 0,4ng/ml, angina instável, risco de morte em 42 dias.
-
Upload
virgiliolazaro -
Category
Documents
-
view
227 -
download
0
Transcript of INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 1/9
INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
� CPK (24 - 195 U/L);� CKMB ( até 16 U/L);
Creatine kinase-MB SI UNITS: 0±7 µg/L CONVENTIONAL UNITS: 0±7 ng/mL
� Troponina T e I;
Troponin I: SI UNITS: 0±0.4 µg/L CONVENTIONAL UNITS: 0±0.4 ng/Ml
Troponin T SI UNITS: 0±0.1 µg/L CONVENTIONAL UNITS: 0±0.1 ng/mL
� Mioglobinas.
Myoglobin S
Male: 19±92 µg/L
Female: 12±76 µg/L
Troponina T� Detectada de 3 a 12 horas após o IAM� No sangue até 10 dias� Níveis de 0,1 a 0,2 ng/ml� Dosar admissão, 4, 8 e 16 horas� Estudo de Peacock et al, com 266 pts,sensibilidade de 9,5% e especificidade de99,2% na predição de eventos adversos.
Troponina I� Não é expressa em músculo esquelético humanodurante o desenvolvimento fetal, após trauma oudurante regeneração da musculatura esquelética.Éaltamente específica para o miocárdio.� No sangue de 7 a 10 dias após a necrose� Estudo de Antman et al, com 1404 pts, 0,4ng/ml,
angina instável, risco de morte em 42 dias.
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 2/9
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 3/9
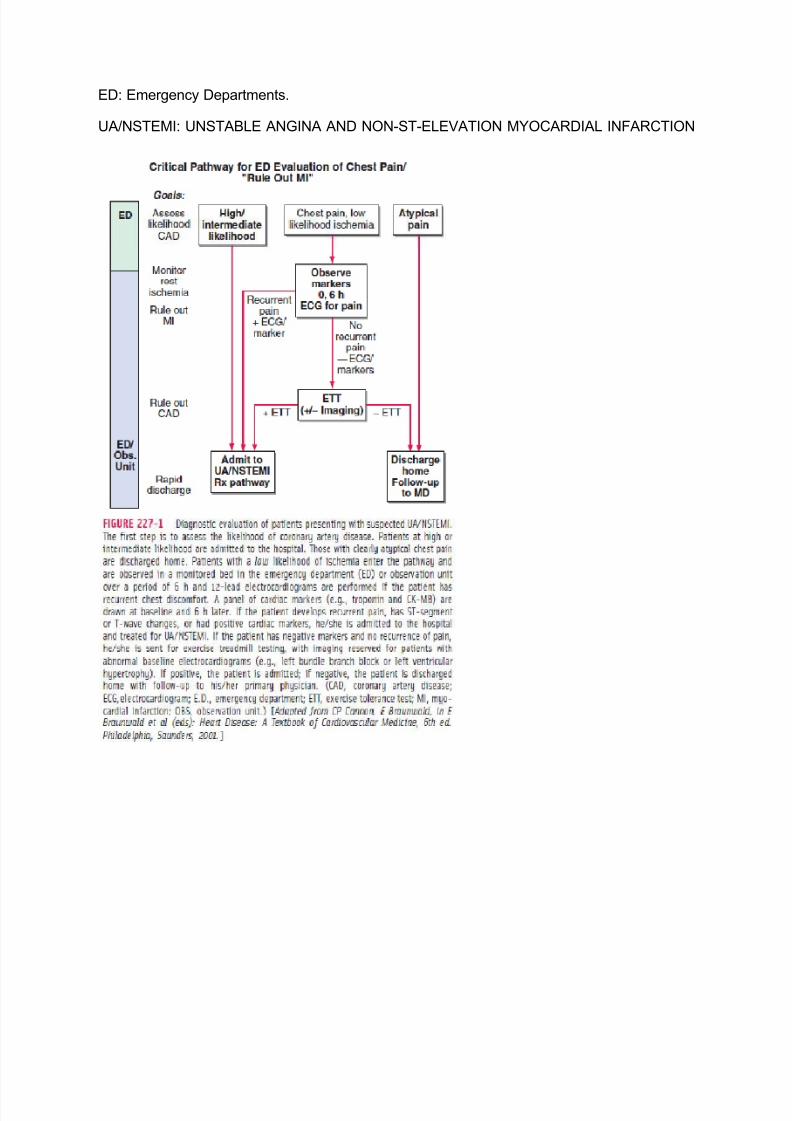
ED: Emergency Departments.
UA/NSTEMI: UNSTABLE ANGINA AND NON-ST-ELEVATION MYOCARDIAL INFARCTION
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 4/9
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 5/9
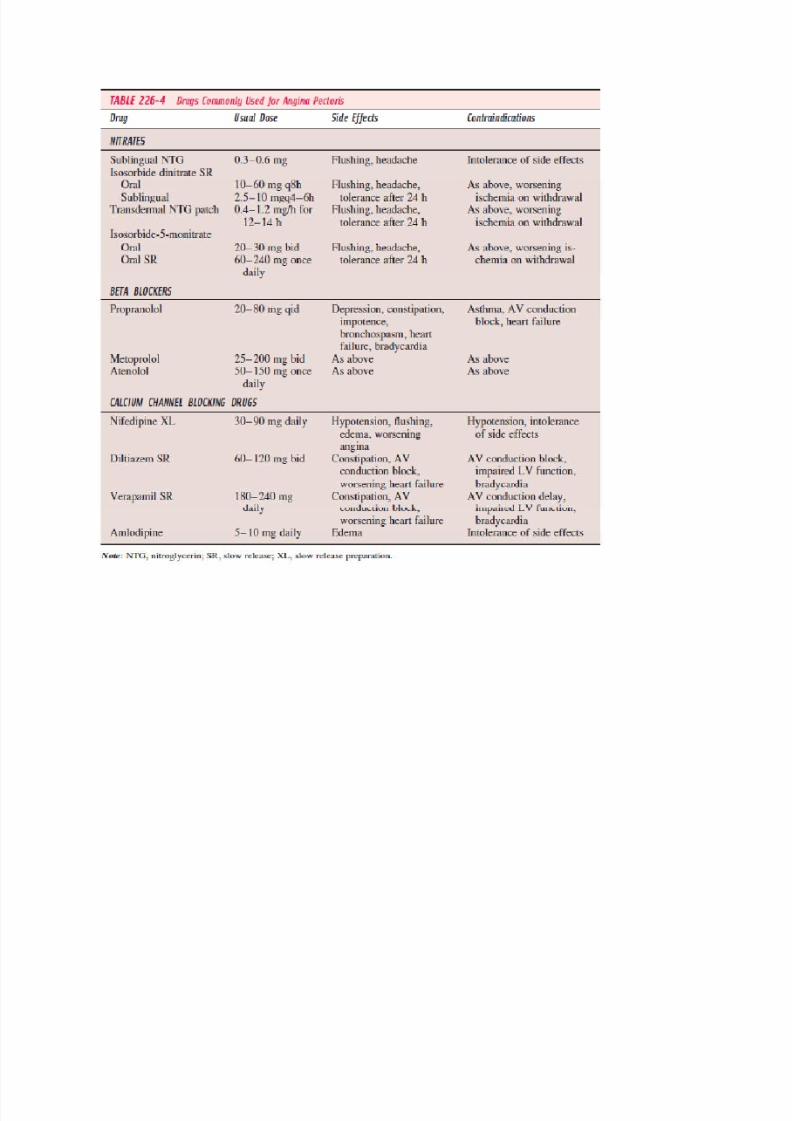
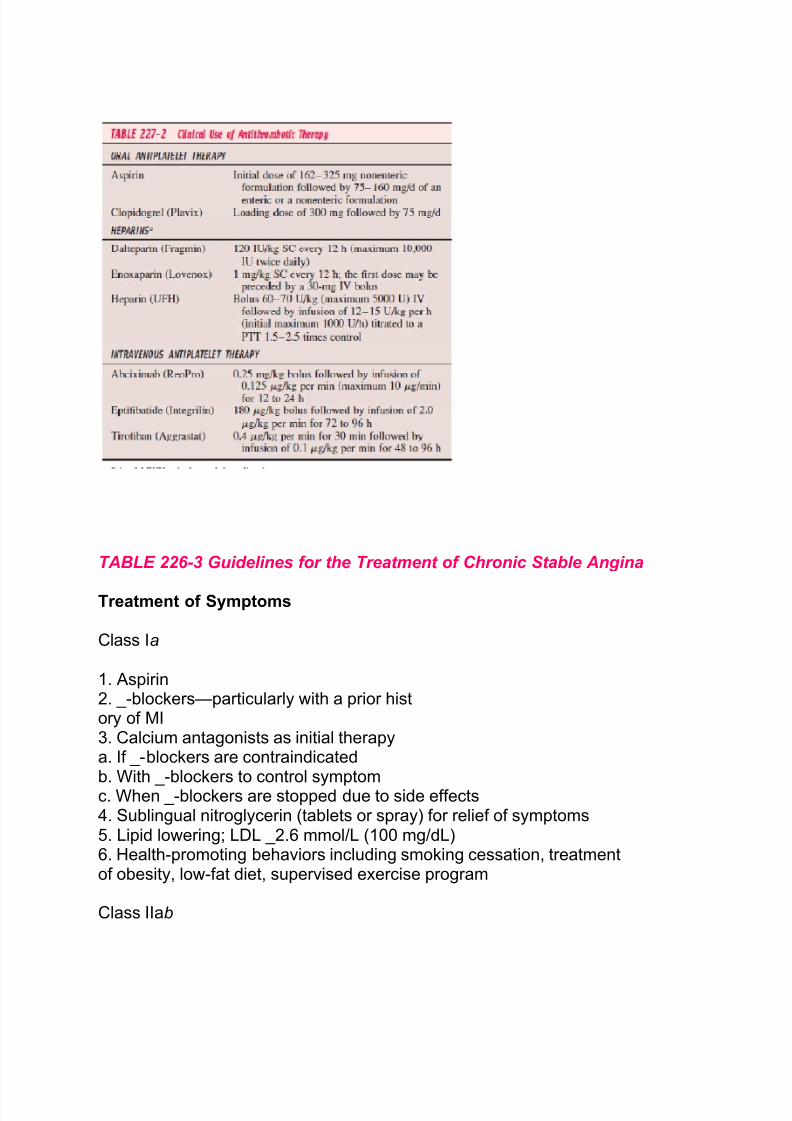
TABLE 226-3 Guidelines for the Treatment of Chronic Stable Angina
Treatment of Symptoms
Class Ia
1. Aspirin2. _-blockers²particularly with a prior history of MI3. Calcium antagonists as initial therapya. If _-blockers are contraindicatedb. With _-blockers to control symptomc. When _-blockers are stopped due to side effects4. Sublingual nitroglycerin (tablets or spray) for relief of symptoms5. Lipid lowering; LDL _2.6 mmol/L (100 mg/dL)6. Health-promoting behaviors including smoking cessation, treatmentof obesity, low-fat diet, supervised exercise program
Class IIab
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 6/9
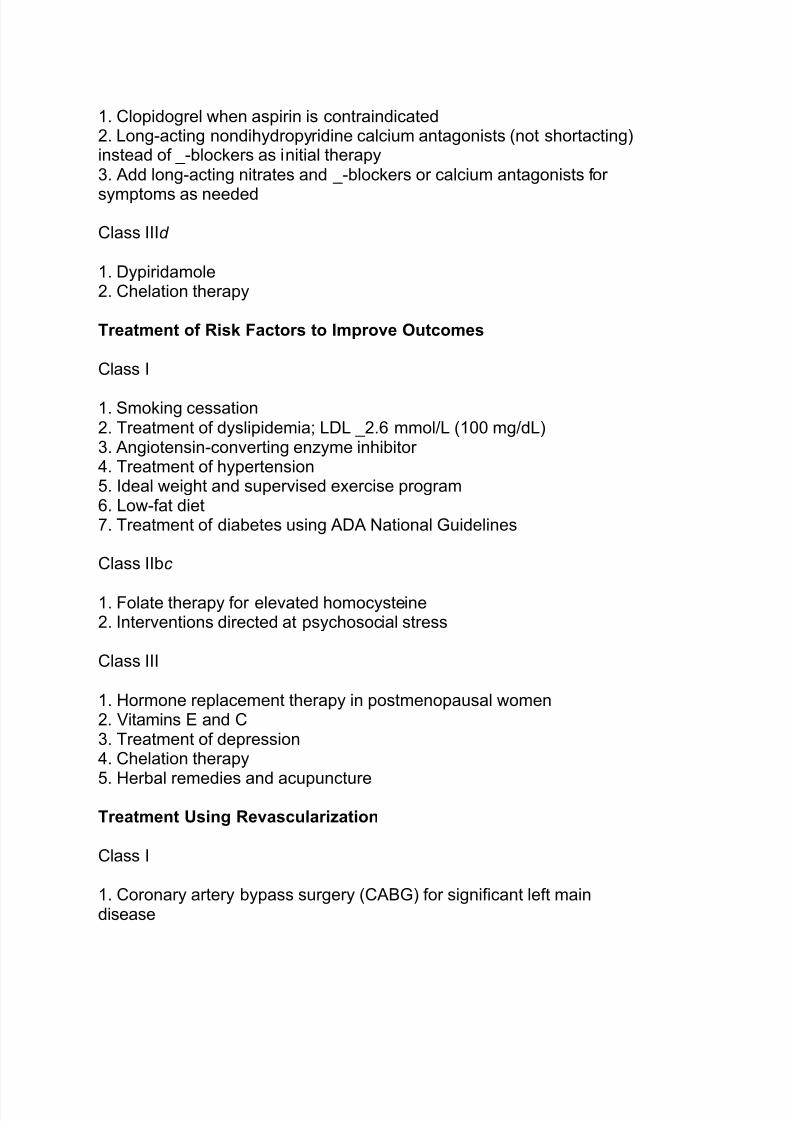
1. Clopidogrel when aspirin is contraindicated2. Long-acting nondihydropyridine calcium antagonists (not shortacting)instead of _-blockers as initial therapy3. Add long-acting nitrates and _-blockers or calcium antagonists for
symptoms as needed
Class IIId
1. Dypiridamole2. Chelation therapy
Treatment of Risk Factors to Improve Outcomes
Class I
1. Smoking cessation2. Treatment of dyslipidemia; LDL _2.6 mmol/L (100 mg/dL)3. Angiotensin-converting enzyme inhibitor 4. Treatment of hypertension5. Ideal weight and supervised exercise program6. Low-fat diet7. Treatment of diabetes using ADA National Guidelines
Class IIbc
1. Folate therapy for elevated homocysteine2. Interventions directed at psychosocial stress
Class III
1. Hormone replacement therapy in postmenopausal women2. Vitamins E and C3. Treatment of depression4. Chelation therapy
5. Herbal remedies and acupunctureTreatment Using Revascularization
Class I
1. Coronary artery bypass surgery (CABG) for significant left maindisease
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 7/9
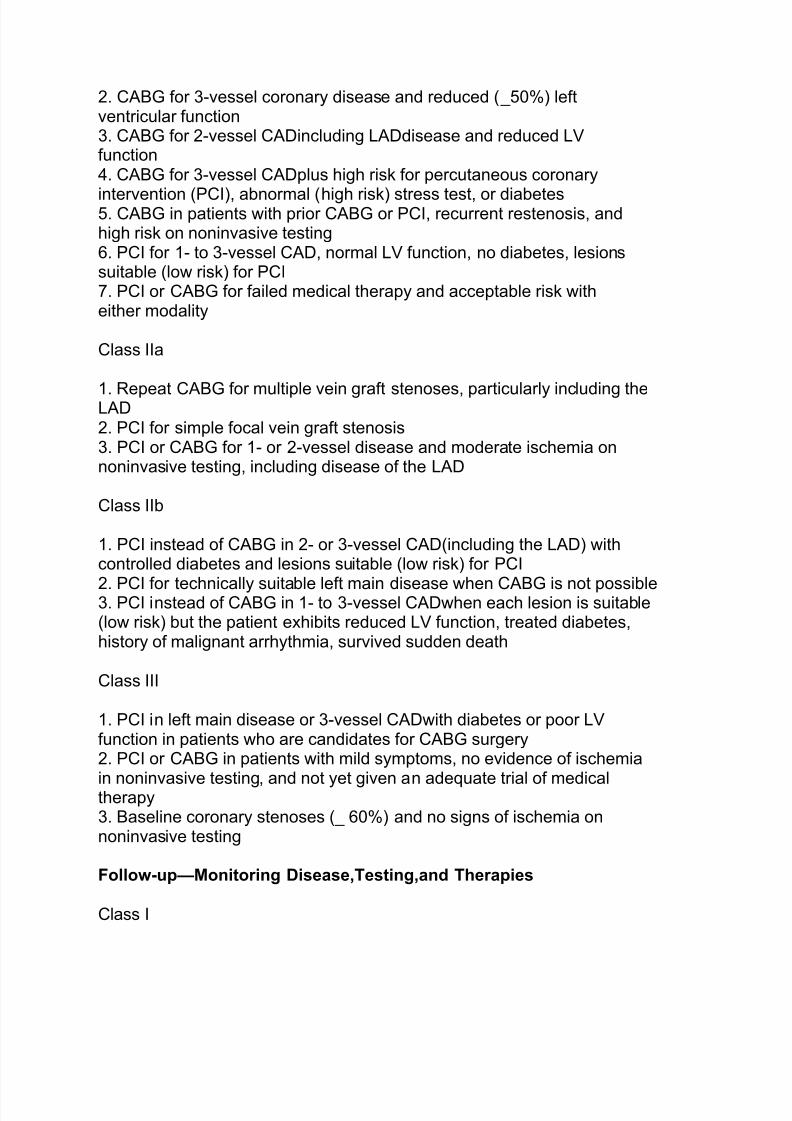
2. CABG for 3-vessel coronary disease and reduced (_50%) leftventricular function3. CABG for 2-vessel CADincluding LADdisease and reduced LVfunction4. CABG for 3-vessel CADplus high risk for percutaneous coronary
intervention (PCI), abnormal (high risk) stress test, or diabetes5. CABG in patients with prior CABG or PCI, recurrent restenosis, andhigh risk on noninvasive testing6. PCI for 1- to 3-vessel CAD, normal LV function, no diabetes, lesionssuitable (low risk) for PCI7. PCI or CABG for failed medical therapy and acceptable risk witheither modality
Class IIa
1. Repeat CABG for multiple vein graft stenoses, particularly including theLAD2. PCI for simple focal vein graft stenosis3. PCI or CABG for 1- or 2-vessel disease and moderate ischemia onnoninvasive testing, including disease of the LAD
Class IIb
1. PCI instead of CABG in 2- or 3-vessel CAD(including the LAD) withcontrolled diabetes and lesions suitable (low risk) for PCI
2. PCI for technically suitable left main disease when CABG is not possible3. PCI instead of CABG in 1- to 3-vessel CADwhen each lesion is suitable(low risk) but the patient exhibits reduced LV function, treated diabetes,history of malignant arrhythmia, survived sudden death
Class III
1. PCI in left main disease or 3-vessel CADwith diabetes or poor LVfunction in patients who are candidates for CABG surgery2. PCI or CABG in patients with mild symptoms, no evidence of ischemia
in noninvasive testing, and not yet given an adequate trial of medicaltherapy3. Baseline coronary stenoses (_ 60%) and no signs of ischemia onnoninvasive testing
Follow-up²Monitoring Disease,Testing,and Therapies
Class I
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 8/9
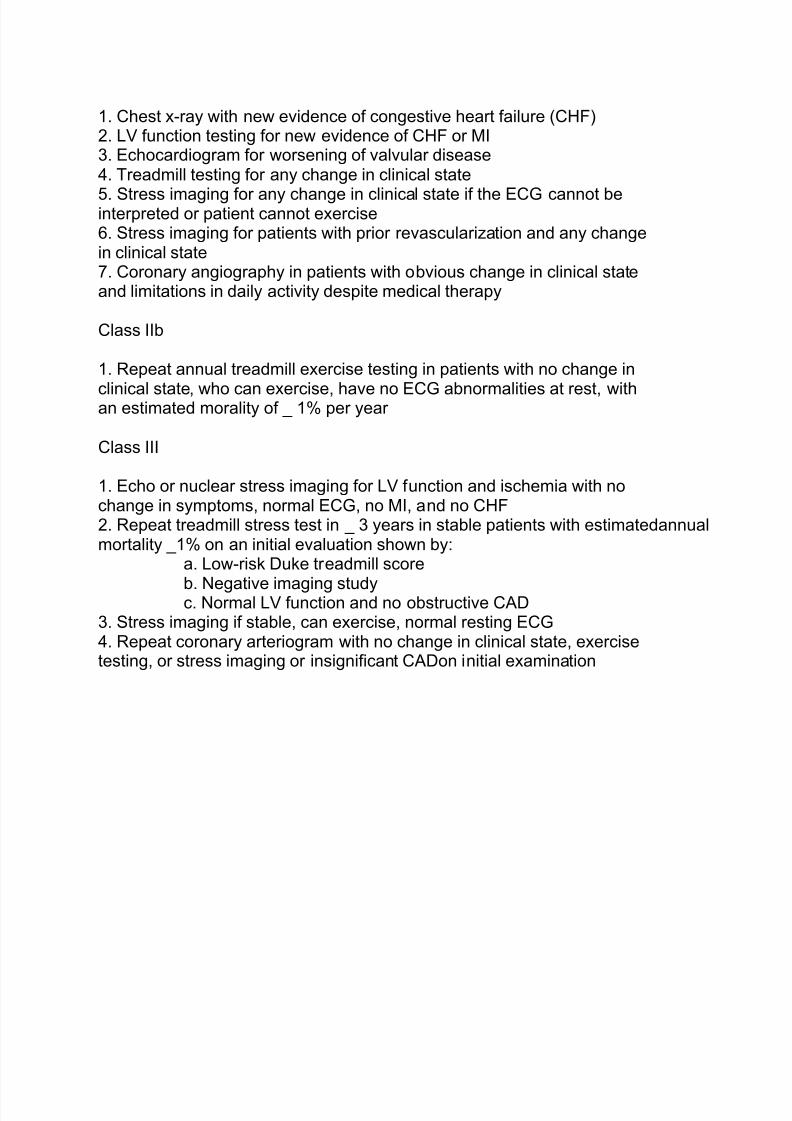
1. Chest x-ray with new evidence of congestive heart failure (CHF)2. LV function testing for new evidence of CHF or MI3. Echocardiogram for worsening of valvular disease4. Treadmill testing for any change in clinical state
5. Stress imaging for any change in clinical state if the ECG cannot beinterpreted or patient cannot exercise6. Stress imaging for patients with prior revascularization and any changein clinical state7. Coronary angiography in patients with obvious change in clinical stateand limitations in daily activity despite medical therapy
Class IIb
1. Repeat annual treadmill exercise testing in patients with no change in
clinical state, who can exercise, have no ECG abnormalities at rest, withan estimated morality of _ 1% per year
Class III
1. Echo or nuclear stress imaging for LV function and ischemia with nochange in symptoms, normal ECG, no MI, and no CHF2. Repeat treadmill stress test in _ 3 years in stable patients with estimatedannualmortality _1% on an initial evaluation shown by:
a. Low-risk Duke treadmill score
b. Negative imaging studyc. Normal LV function and no obstructive CAD3. Stress imaging if stable, can exercise, normal resting ECG4. Repeat coronary arteriogram with no change in clinical state, exercisetesting, or stress imaging or insignificant CADon initial examination
8/6/2019 INFARTO AGUDO DO MIOCÁRDIO ENZIMAS CARDÍACAS
http://slidepdf.com/reader/full/infarto-agudo-do-miocardio-enzimas-cardiacas 9/9
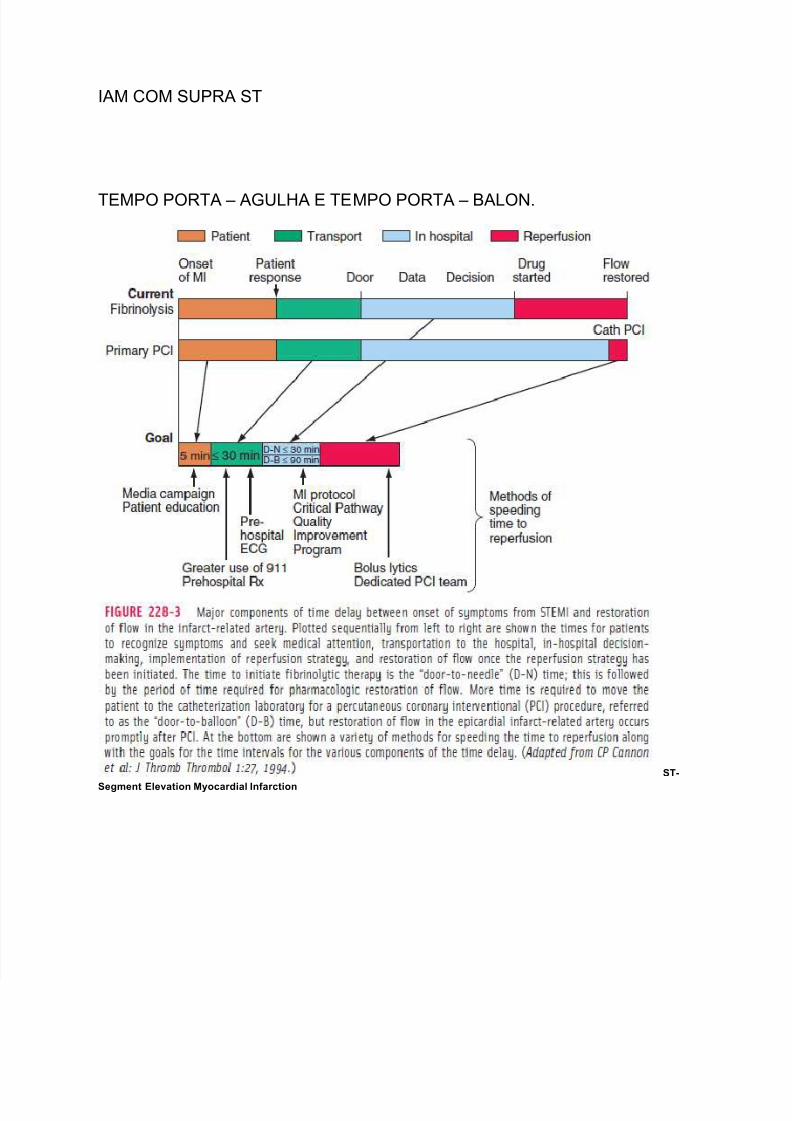
IAM COM SUPRA ST
TEMPO PORTA ± AGULHA E TEMPO PORTA ± BALON.
ST-
Segment Elevation Myocardial Infarction















![BRILINTA ticagrelor I) IDENTIFICAÇÃO DO MEDICAMENTO ... · BRILINTA é indicado para a prevenção de eventos trombóticos (morte cardiovascular [CV], infarto do miocárdio [IM]](https://static.fdocuments.ec/doc/165x107/5fc7a0e645d22b062c00b898/brilinta-ticagrelor-i-identificafo-do-medicamento-brilinta-indicado-para.jpg)