
Impact of Laparoscopic Sleeve Gastrectomy on...
18
Review Article Impact of Laparoscopic Sleeve Gastrectomy on Gastrointestinal Motility Eleni Sioka, George Tzovaras, Konstantinos Perivoliotis , Vissarion Bakalis, Eleni Zachari, Dimitrios Magouliotis, Vassiliki Tassiopoulou, Spyridon Potamianos, Andreas Kapsoritakis, Antigoni Poultsidi, Konstantinos Tepetes , Constantine Chatzitheofilou, and Dimitris Zacharoulis Department of Surgery, University Hospital of Larissa, Larissa, Greece Correspondence should be addressed to Dimitris Zacharoulis; [email protected] Received 24 December 2017; Accepted 4 March 2018; Published 5 April 2018 Academic Editor: Riccardo Casadei Copyright © 2018 Eleni Sioka et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objective. Laparoscopic sleeve gastrectomy (LSG) was considered mainly as a restrictive procedure due to anatomic alterations in the upper gastrointestinal tract. Additionally, due to neurohormonal alterations, LSG modifies the gastrointestinal motility, which controls appetite and feeling of satiety. Aim. The aim of the study was to review the impact of laparoscopic sleeve gastrectomy on gastrointestinal motility. Material and Methods. A search of the medical literature was undertaken in Pubmed, Web of Science, and Cochrane library. Esophageal, gastric, bowel motility were assessed separately. Results. Nine studies assessed esophageal motility. The data remain debatable attributing to the heterogeneity of follow-up timing, surgical technique, bougie size, and distance from pylorus. The stomach motility was assessed in eighteen studies. Functionally, the sleeve was divided into a passive sleeve and an accelerated antrum. All scintigraphic studies revealed accelerated gastric emptying after LSG except of one. Patients demonstrated a rapid gastroduodenal transit time. The resection of the gastric pacemaker had as a consequence aberrant distal ectopic pacemaking or bioelectrical quiescence after LSG. The bowel motility was the least studied. Small bowel transit time was reduced; opposite to that the initiation of cecal filling and the ileocecal valve transit was delayed. Conclusion. Laparoscopic sleeve gastrectomy has impacts on gastrointestinal motility. The data remain debatable for esophageal motility. Stomach and small bowel motility were accelerated, while the initiation of cecal filling and the ileocecal valve transit was delayed. Further pathophysiological studies are needed to evaluate the correlation of motility data with clinical symptoms. 1. Introduction Laparoscopic sleeve gastrectomy (LSG) is the most fre- quently performed procedure in the world and has overtaken the “gold standard” Roux-en-Y gastric bypass (RYGB), which remains the most performed bariatric/metabolic procedure only in Latin/South America. The trend analysis demonstrated that LSG had the largest average annual percentage increase of approximately 9% from 2013 of the worldwide bariatric/metabolic surgical procedures [1]. Lapa- roscopic sleeve gastrectomy is positioned between the adjust- able gastric banding and RYGB in terms of morbidity with effectiveness comparable to RYGB even at five years [2, 3]. Laparoscopic sleeve gastrectomy involves the removal of the gastric fundus and greater curvature portion of the stomach, leaving only a lesser curvature tube. Yehoshua et al. showed that after the sleeve, the fundus, which is the most distensible part of the stomach, is removed, thus leaving a sleeve which is characterized by markedly lesser distensibil- ity and high intraluminal pressure, leading to the feeling of early satiety [4]. The abstraction of the fundus is related to physiological alterations in the upper gastrointestinal tract, since the angle of His and the receptive relaxation mecha- nism is abolished, and the gastric pacemaker is abandoned. Furthermore, the antrum is preserved in some cases depend- ing on the distance of the resection, and the pylorus remains Hindawi Gastroenterology Research and Practice Volume 2018, Article ID 4135813, 17 pages https://doi.org/10.1155/2018/4135813
Transcript of Impact of Laparoscopic Sleeve Gastrectomy on...

Review ArticleImpact of Laparoscopic Sleeve Gastrectomy onGastrointestinal Motility
Eleni Sioka, George Tzovaras, Konstantinos Perivoliotis , Vissarion Bakalis, Eleni Zachari,Dimitrios Magouliotis, Vassiliki Tassiopoulou, Spyridon Potamianos, Andreas Kapsoritakis,Antigoni Poultsidi, Konstantinos Tepetes , Constantine Chatzitheofilou,and Dimitris Zacharoulis
Department of Surgery, University Hospital of Larissa, Larissa, Greece
Correspondence should be addressed to Dimitris Zacharoulis; [email protected]
Received 24 December 2017; Accepted 4 March 2018; Published 5 April 2018
Academic Editor: Riccardo Casadei
Copyright © 2018 Eleni Sioka et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective. Laparoscopic sleeve gastrectomy (LSG) was considered mainly as a restrictive procedure due to anatomic alterations inthe upper gastrointestinal tract. Additionally, due to neurohormonal alterations, LSG modifies the gastrointestinal motility, whichcontrols appetite and feeling of satiety. Aim. The aim of the study was to review the impact of laparoscopic sleeve gastrectomy ongastrointestinal motility.Material and Methods. A search of the medical literature was undertaken in Pubmed, Web of Science, andCochrane library. Esophageal, gastric, bowel motility were assessed separately. Results. Nine studies assessed esophageal motility.The data remain debatable attributing to the heterogeneity of follow-up timing, surgical technique, bougie size, and distancefrom pylorus. The stomach motility was assessed in eighteen studies. Functionally, the sleeve was divided into a passive sleeveand an accelerated antrum. All scintigraphic studies revealed accelerated gastric emptying after LSG except of one. Patientsdemonstrated a rapid gastroduodenal transit time. The resection of the gastric pacemaker had as a consequence aberrant distalectopic pacemaking or bioelectrical quiescence after LSG. The bowel motility was the least studied. Small bowel transit time wasreduced; opposite to that the initiation of cecal filling and the ileocecal valve transit was delayed. Conclusion. Laparoscopic sleevegastrectomy has impacts on gastrointestinal motility. The data remain debatable for esophageal motility. Stomach and smallbowel motility were accelerated, while the initiation of cecal filling and the ileocecal valve transit was delayed. Furtherpathophysiological studies are needed to evaluate the correlation of motility data with clinical symptoms.
1. Introduction
Laparoscopic sleeve gastrectomy (LSG) is the most fre-quently performed procedure in the world and has overtakenthe “gold standard” Roux-en-Y gastric bypass (RYGB),which remains the most performed bariatric/metabolicprocedure only in Latin/South America. The trend analysisdemonstrated that LSG had the largest average annualpercentage increase of approximately 9% from 2013 of theworldwide bariatric/metabolic surgical procedures [1]. Lapa-roscopic sleeve gastrectomy is positioned between the adjust-able gastric banding and RYGB in terms of morbidity witheffectiveness comparable to RYGB even at five years [2, 3].
Laparoscopic sleeve gastrectomy involves the removal ofthe gastric fundus and greater curvature portion of thestomach, leaving only a lesser curvature tube. Yehoshuaet al. showed that after the sleeve, the fundus, which is themost distensible part of the stomach, is removed, thus leavinga sleeve which is characterized by markedly lesser distensibil-ity and high intraluminal pressure, leading to the feeling ofearly satiety [4]. The abstraction of the fundus is related tophysiological alterations in the upper gastrointestinal tract,since the angle of His and the receptive relaxation mecha-nism is abolished, and the gastric pacemaker is abandoned.Furthermore, the antrum is preserved in some cases depend-ing on the distance of the resection, and the pylorus remains
HindawiGastroenterology Research and PracticeVolume 2018, Article ID 4135813, 17 pageshttps://doi.org/10.1155/2018/4135813

intact. These physiological changes are expected to provokemotility alterations at the gastrointestinal tract.
The aim of the study was to review the impact of laparo-scopic sleeve gastrectomy on gastrointestinal motility.
2. Material and Methods
2.1. Search Strategy. A search of the medical literature wasundertaken in Pubmed, Web of Science, and Cochranelibrary until August 2017. The keywords used were “sleevegastrectomy” AND (motility OR gastrointestinal motilityOR esophageal motility OR gastric motility OR bowel motil-ity OR emptying OR manometry).
2.2. Eligibility Criteria
2.2.1. Types of Studies. All studies assessing the impact ofLSG on gastrointestinal motility were included. Esophageal,stomach, and bowel motilities were assessed separately.
2.2.2. Types of Participants. The types of participantswere obese patients (BMI > 30) undergoing laparoscopicsleeve gastrectomy.
2.2.3. Types of Outcome Measures. The outcomes measuredwere esophageal, gastric, and bowel motility.
2.3. Inclusion and Exclusion Criteria. Two independentreviewers (Eleni Sioka and Konstantinos Perivoliotis) screenedabstracts, reviewed full text versions of all studies classified,and extracted data. Any trial considered relevant wasretrieved for further review. The full texts were indepen-dently assessed by two reviewers. Disagreements wereresolved with a third reviewer. Only published articles inthe English language were included. Meta-analysis, system-atic reviews, letters to the editor, case studies, non-Englishlanguage publications, duplicate studies, experimentalstudies, and conference papers were excluded.
2.4. Data Extraction and Quality Assessment. One reviewer(Konstantinos Perivoliotis) extracted data from selected trialsand a second reviewer (Eleni Sioka) checked for accuracy.The data were standardized and extracted from each study,and data were recorded into a database. The variables col-lected were first author, year of publication, country, type ofstudy, number of participants, method of assessment, timingpoints, and main findings.
3. Results
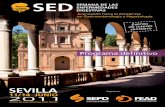
3.1. Study Selection. One hundred seventy eight studies werescreened for eligibility and fifty two studies assessed in fulltext. Twenty four studies were excluded due to various rea-sons. Finally, 28 studies were eligible to be included in thereview (Figure 1). There was complete agreement amongthe authors as to the inclusion of these studies.
3.2. Esophageal Motility. Nine studies assessed esophagealmotility. Two studies were conducted in Greece [5, 6], onein France [7], two in Italy [8, 9], one in Argentina [10], one
in Netherlands [11], one in Germany [12], aand one in Chile[13]. All except of one [7] were prospective studies.
The postoperative follow-up ranged from 6 days to 50months. The bougie size ranged from 32 to 40F. The distancefrom the pylorus ranged from 2 to 6 cm. The lower esoph-ageal sphincter (LES) length was reduced in three studies[5, 9, 13] increased in two studies [6, 10], and unchangedin one study [8]. The LES resting pressure decreased infour studies [5, 10, 11, 13], increased in two studies [6, 12],and remained unchanged in two studies [8, 9]. The ampli-tude pressure was reduced in two studies [5, 11], increasedin one study [10], and unchanged in one study [8]. Ampli-tude pressure decreased in distal esophagus and increasedin the other parts in one study [6]. Ineffective motility wasreported in four studies. The percentage was increased from10% to 45% postoperatively in one study [9], while it wasthe same preoperatively (7%) in another study [10], wasincreased at 5% (1/20 patients) in one study [11], and wasreported at 37.7% (20/53 patients) in another study [7]. The
91 recordsidentified
through MEDLINE
15 recordsidentifiedthrough
CENTRAL
74 duplicates removed
178 recordsscreened
52 full-textarticles assessed
for eligibility
24 full-text articlesexcluded
28 studiesincluded in
qualitative andquantitative
synthesis
126 recordsexcluded
9 nonhumanstudies
3 non-Englisharticles
59reviews/conference
abstracts55 irrelevant
records
9 articlesconcerning
esophageal motility18 articles
concerning gastricmotility3 articles
concerning bowelmotility
24 irrelevant studies
146 recordsidentified
through Web ofScience
Figure 1: Flow diagram.
2 Gastroenterology Research and Practice

percentage of normal peristaltic contractions was not affectedin one study [11], while it increased in another study [5]. Thesummary of studies is reported in Table 1.
3.3. Stomach Motility. Eighteen studies assessed stomachmotility. Eleven studies were conducted in Europe (Spain[n = 2] [14, 15], Italy [n = 3] [16–18], Greece [n = 3][19–21], Czech Republic [n = 1] [22], Germany [n = 1] [23],and the Netherlands [n = 1] [24]), whereas one study wasperformed in the USA [25], two studies in India [26, 27],one study in New Zealand [28], one in Egypt [29], one inChile [30], and one in Israel [31]. Twelve studies were pro-spective studies, four studies were prospective randomizedcontrolled studies [14, 17, 22, 27], and two were retrospectivestudies [18, 25]. The method of gastric emptying assessmentwas gastric scintigraphic studies in fourteen studies andmagnetic resonance imaging (MRI) in one study [23], whileone study assessed the gastric slow-wave pacemaking usinglaparoscopic high-resolution (HR) electrical mapping [28],and two studies assessed the gastroduodenal transit time byradiological upper gastrointestinal series [18, 25].
The postoperative follow-up ranged from 3 to 24months.The bougie size ranged from 32 to 48F. The distance fromthe pylorus ranged from 2 to 8 cm. All studies showedaccelerated gastric emptying after LSG except for one[31]. Functionally, the sleeve was divided into a passivesleeve and an accelerated antrum. The patients demon-strated a rapid gastroduodenal transit time. The resectionof the gastric pacemaker had as a consequence aberrant dis-tal ectopic pacemaking or bioelectrical quiescence after LSG.No correlation was observed between gastric emptying andpostprandial symptoms in one study. No correlation wasfound between gastroduodenal transit time and weight lossin one study [25], while in another study, patients showinga rapid gastroduodenal transit had better weight loss thanpatients presenting with a slow voiding rate [18]. Thesummary of the studies are presented in Table 2.
3.4. Bowel Motility. Three studies assessed the bowel motility.Two were prospective studies and one was prospectiverandomized study. One study was conducted in Japan, onein Greece, and one in India [21, 27, 32]. Trung et al. evaluatedthe intestinal motility using cine MRI preoperatively and 3months postoperatively and found reduced intestinal transittime leading to accelerated intestinal motility [32]. Melissaset al. evaluated prospectively 21 patients preoperatively witha g-camera and 4 months postoperatively. Apart from theacceleration of small bowel transit time, the authors showedthat initiation of cecal filling and the ileocecal valve transitwas delayed [21]. Similarly, Shah et al. showed decreasedsmall bowel transit time after LSG [27] (Table 3).
4. Discussion
The aim of this study was to review the impact of laparo-scopic sleeve gastrectomy on gastrointestinal motility. Thegastrointestinal motility research might be essential to recog-nize the behavior of the created sleeve, to explain possibleclinical symptoms-implications, and to elucidate possible
mechanisms of actions of this procedure. According to theSecond International Consensus Summit for Sleeve Gastrec-tomy, the panel of experts voted the following as mechanismsof action: restriction: 79%, gastric emptying: 0%, hormonal:16%, malabsorption: 0%, and other: 3% [33]. Since 2007,LSG was characterized as more than a restrictive procedure[19]. Additional supportive evidence came from studiesassessing hormonal alterations after LSG. Concerning hor-monal changes, it seems that patients experienced a pro-nounced and long-lasting decrease of circulating ghrelinand increased postprandial release of the CCK, GLP-1, andPYY, the so-called gut peptides after LSG. It was hypothe-sized that the faster delivery of nutrients to the distalintestinal tract postoperatively may provoke increased thepostprandial release of the gut peptides contributing to theimprovement of glucose control as well as to the reductionof food intake and subsequently body weight [34].
The esophageal motility was assessed in several studies.The limitations of the studies include the small sample size.The data remain debatable. The variability in the outcomesof esophageal motility may be attributable to the timing ofpostoperative follow-up, the variability of surgical tech-niques, the different bougie sizes, and the different dissec-tions from pylorus, thus creating a sleeve with variabledistensibility and intraluminal pressure with, in part, thepreservation of the antrum. The percentage of peristalticnormal contractions increased postoperatively and is notstatistically significant at 3 months [11] but statisticallysignificant later [5]. It seems that the motility of the body ofthe esophagus was normalized. Perhaps, this might beattributable to the reduced intrabdominal pressure due toweight loss. An increase in the esophageal acidification wasreported in few studies [9, 11]. Del Genio et al. pointedout a decrease in the esophageal transit after LSG inimpedance study. Furthermore, the authors explained thereflux episodes as a consequence of retrograde movementsinto the esophagus [9].
Gastric motility emerges as the role of the stomach as anendocrine organ. Gastric motility acts as a central mediatorof hunger, satiation, and satiety. Gastric emptying plays akey role in regulating food intake. Gastric distention acts asatiety signal to inhibit food intake [35]. During food intake,it is the gastric distention and gastric accommodation thatregulate satiation in a manner. After food intake, when thestomach empties gradually, it is the gastric emptying andthe intestinal exposure of the nutrients that play a key role,while the role of gastric distention follows. It seems thatgastric accommodation and gastric emptying are implicatedin the regulation of gastric distention and intestinal exposureof nutrients, thus control satiation and satiety. The correla-tions between gastric accommodation, gastric emptying,and body weight suggest that gastric motility may also affectthe long-term regulation of body weight [36].
A number of studies assessed gastric motility. Baumannet al. showed that the sleeve was completely motionlesswithout any coordinate peristalsis, while the antrum hadfaster peristaltic folds, concluding that gastric emptying isdirectly linked to the function of the antrum when theantrum is preserved in LSG [23]. It seems that the resection
3Gastroenterology Research and Practice

Table1:Stud
iesassessingesop
hagealmotility.
No.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients
Metho
dof
assessment/
follow-up
Distancefrom
pylorus/bougiesize
Mainfind
ings
ofthestud
y
1Sioka,E.etal.,
2017
[5],Greece
Prospective
stud
y18
Esoph
agealm
anom
etry
preoperativelyandat
medianintervalof
7mon
ths
5cm
/36F
The
lower
esop
hagealsphincter(LES)
totallengthdecreased
postop
eratively(p
=0002).T
herestingandresidu
alpressurestend
edto
decrease
postop
eratively(m
ean
difference
[95%
confi
denceinterval]:−4
[−8.3/0.2]
mmHg,
p=0 0
60;−
1.4[−3/0.1]
mmHg,p=0071,resp.).T
heam
plitud
epressure
decreasedfrom
95.7±37.3to
69.8±26.3mmHgattheup
perborderofLE
S(p
=0 0
14)and
tend
edto
decrease
atthedistalesop
hagusfrom
128.5±30.1
to112.1±3
5.4mmHg(p
=006)andmidesop
hagusfrom
72.7±34.5to
49.4±16.7mmHg(p
=0 0
06).The
peristaltic
norm
alsw
allowpercentage
increasedfrom
47.2±36.8to
82.8±28%
(p=0 0
03).The
postop
erativeregurgitationwas
stronglynegativelycorrelated
withLE
Stotallength
(Spearman’sr=−0
670).W
hengrou
pswerecompared
accordingto
heartburnstatus,the
statisticalsignificancewas
observed
betweenthegrou
psof
improvem
entand
deteriorationregardingpo
stop
erativeresidu
alpressure
and
postop
erativerelaxation
(p<0002a
ndp<0002,resp.).
Withregard
toregurgitationstatus,there
was
statistically
significant
difference
betweengrou
psregardingpreoperative
amplitud
epressure
attheup
perborder
ofLE
S(p
<0056).
PatientsdevelopeddecreasedLE
Slength
andweakenedLE
Spressure
afterLSG.E
soph
agealb
odyperistalsiswas
also
affectedin
term
sof
decreasedam
plitud
epressure,especially
attheup
perborderofLE
S.Nevertheless,body
peristalsiswas
norm
alized
postop
eratively.LSGmight
notdeteriorate
heartburn.
Regurgitation
might
increase
followingLSGdu
eto
shortening
ofLE
Slength,p
articularlyin
patientswith
rangeofpreoperative
amplitud
epressureattheup
perborder
ofLE
Sof
38.9–92.6mmHg.
2Mion,
F.etal.,
2016
[7],France
Retrospective
stud
y53
High-resolution
impedancemanom
etry
Sleeve
volumeand
diam
eter
withCTscan
Medianfollow-upat
11mon
ths(1–50)
NR/N
R
The
increasedintragastricpressure
occurred
very
frequently
inpatientsafterSG
(77%
)andwas
notassociated
withany
upperGIsymptom
s,specificesop
hagealmanom
etricprofi
le,
orim
pedancereflux.Impedancereflux
episod
eswerealso
frequentlyobserved
afterSG
(52%
):they
weresignificantly
associated
withgastroesop
hagealreflux
(GER)symptom
sandineffective
esop
hagealmotility.T
hesleeve
volumeand
diam
eterswerealso
significantlysm
allerin
patientswith
impedancereflux
episod
es(p
<001).
4 Gastroenterology Research and Practice

Table1:Con
tinu
ed.
No.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients
Metho
dof
assessment/
follow-up
Distancefrom
pylorus/bougiesize
Mainfind
ings
ofthestud
y
SGsignificantlymod
ified
esop
hagogastricmotility.T
heIIGP
isfrequent,n
otcorrelated
tosymptom
sandshou
ldbe
regarded
asaHRIM
markerof
SG.T
heim
pedancereflux
episod
eswerealso
frequent,associatedwithGERsymptom
sandesop
hagealdysm
otility.H
RIM
may
thus
have
aclinical
impacton
themanagem
entof
patientswithup
perGI
symptom
safterSG
.
3Rebecchi,F.
etal.,
2014
[8],Italy
Prospective
clinicalstud
y65
Clin
icallyvalid
ated
question
naire,up
per
endo
scop
y,esop
hageal
manom
etry,and
24-hou
rpH
mon
itoringbefore
and
24mon
thsafterLSG.
6cm
/36F
Onthebasisof
preoperative
24-hou
rpH
mon
itoring,
patientsweredividedinto
grou
pA(patho
logic,n=28)and
grou
pB(normal,n
=37).The
symptom
sim
proved
ingrou
pA,w
iththegastroesop
hagealreflux
diseasesymptom
assessmentscalescoredecreasing
from
53.1±10.5to
13.1±3.5(p
<0001).T
heDeM
eester
scoreandtotalacid
expo
sure
(%pH
<4)
decreasedin
grou
pApatients
(DeM
eester
scorefrom
39.5±16.5to
10.6±5.8,p<0 0
01;
%pH
<4from
10.2±3.7to
4.2±2.6,p<00
01).Reald
eno
voGERDoccurred
in5.4%
ofgrou
pBpatients.N
osignificant
changesin
thelower
esop
hagealsphincter
pressure
andesop
hagealperistalsisam
plitud
ewerefoun
din
both
grou
ps.
LSGim
proves
symptom
sandcontrolsreflux
inmost
morbidlyobesepatientswithpreoperative
GERD.Inobese
patientswitho
utpreoperative
evidence
ofGERD,the
occurrence
ofde
novo
reflux
isun
common
.Therefore,L
SGshou
ldbe
considered
asan
effective
option
forthesurgical
treatm
entof
obesepatientswithGERD.
4Gorod
ner,V.
etal.,2015
[10],
Argentina
Prospective
stud
y14
Esoph
agealm
anom
etry
(EM)and24
hpH
mon
itoringbefore
and
1year
afterLSG.
6cm
/36F
The
lower
esop
hagealsphincter(LES)
length
increasedfrom
2.7to
3.2cm
(p=NS
),andLE
Spressure
decreasedfrom
17.1to
12.4mmHg(p
≤005).Preop
eratively,LE
Swas
norm
otensive
in13
(93%
)patients;postoperatively,LESwas
norm
alin
10(71%
)(p
=NS
).After
LSG,the
LESP
significantlydecreased
5Burgerhart,J.S.
etal.,2014
[11],
Netherlands
Prospective
stud
y20
Esoph
agealfun
ctiontests
(high-resolution
manom
etry
(HRM),24-h
pH/impedancemetry)
before
and3mon
ths
afterLSG
6cm
/34F
Esoph
agealacidexpo
sure
significantlyincreasedafter
sleeve
gastrectom
y:up
rightfrom
5.1±4.4to
12.6±9.8%
(p=0 0
03),supine
from
1.4±2.4to11
±15%(p
=00
03)and
totalacidexpo
sure
from
4.1±3.5to
12±10.4%
(p=0 0
04).
The
percentage
ofno
rmalperistalticcontractions
remained
unchanged,bu
tthedistalcontractile
integraldecreasedafter
LSGfrom
2006.0±1806.3to
1537.4±1671.8mmHg·cm·s
(p=001).The
lower
esop
hagealsphincter(LES)
pressure
decreasedfrom
18.3±9.2to
11.0±7.0mmHg(p
=0 0
2).
5Gastroenterology Research and Practice

Table1:Con
tinu
ed.
No.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients
Metho
dof
assessment/
follow-up
Distancefrom
pylorus/bougiesize
Mainfind
ings
ofthestud
y
After
LSG,the
patientshave
significantlyhigher
esop
hageal
acidexpo
sure,w
hich
may
wellbedu
etoadecreaseintheLE
Srestingpressure
followingtheprocedure.
6DelGenio,J.etal.,
2014
[9],Italy
Prospective
stud
y25
High-resolution
impedancemanom
etry
(HRiM
)andcombined
24hpH
andmultichannel
intralum
inalim
pedance
(MII-pH).
Medianfollow-upat
13mon
ths
NR/40F
Unchanged
LESfunction
,increased
ineffective
peristalsis,
andincompletebolustransit.MII-pH
show
edan
increase
ofboth
acid
expo
sure
oftheesop
hagusandnu
mberof
nonacid
reflux
eventsin
postprandialperiod
s.Laparoscop
icSG
isan
effective
restrictiveprocedurethat
createsdelayedesop
hagealem
ptying
witho
utim
pairingLE
Sfunction
.Acorrectlyfashionedsleeve
does
notindu
cede
novo
GERD.R
etrogrademovem
entsandincreasedacid
expo
sure
areprobablydu
eto
stasisandpo
stprandial
regurgitation.
7Kleidi,E.etal.,
2013
[6],Greece
Prospective
stud
y23
Esoph
agealm
anom
etry
preoperativelyand6weeks
postop
eratively
3-4cm
/34F
The
LEStotaland
abdo
minallengthsincreasedsignificantly
postop
eratively,whereas
thecontractionam
plitud
ein
the
lower
esop
hagusdecreased.
There
was
anincrease
inreflux
symptom
spo
stop
eratively(p
<0009).T
heapproxim
ationof
theangleof
Hismostlyfrom
theop
eratingsurgeonresulted
inan
increasedabdo
minalLE
Slength
(p<001).The
presence
ofesop
hagealtissue
inthespecim
encorrelated
with
theincreasedtotalG
ERD
score(p
<005).
LSGweakens
thecontractionam
plitud
eof
thelower
esop
hagus,which
may
contribu
teto
postop
erativereflux
deterioration.
Italso
increasesthetotaland
theabdo
minal
lengthsof
theLE
S,especiallywhentheangleof
Hisismostly
approxim
ated.H
owever,ifthisapproxim
ationleadsto
esop
hagealtissue
excision
,the
reflux
isagainaggravated.
Thu
s,staplin
gtoocloseto
theangleof
Hisshou
ldbe
done
cautiously.
8Petersen,
W.V
.etal.,2012
[12],
Germany
Prospective
stud
y
37Group
I(BMI=
19–2
5)20
(con
trol
grou
p)Group
II(BMI=
42–6
5)20
patients
(8mon
ths)
Group
III
(BMI=
37–5
7)17
patients
(6days)
Esoph
agealm
anom
etry
2cm
/35Ch
Postoperatively,the
LESP
increasedsignificantly,n
amely,
from
preoperative
8.4to
21.2mmHgin
grou
pIIandfrom
11to
24mmHg(p
<00001)in
grou
pIII.The
tubu
lar
esop
hagealmotility
profi
tsfrom
LSG.
The
LSGsignificantlyincreasedthelower
esop
hageal
pressure
independ
entof
weightloss
afterLSGandmay
protectobesepatientsfrom
gastroesop
hagealreflux.
6 Gastroenterology Research and Practice

Table1:Con
tinu
ed.
No.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients
Metho
dof
assessment/
follow-up
Distancefrom
pylorus/bougiesize
Mainfind
ings
ofthestud
y
9Braghetto,I.etal.,
2010
[13],C
hile
Prospective
stud
y20
Esoph
agealm
anom
etry
preoperatively,6
mon
ths
postop
eratively
2cm
/32F
Preop
erativemeanLE
SPwas
14.2±5.8mmHg.The
postop
erativemanom
etry
decreasedin
17/20(85%
),witha
meanvalueof
11.2±5.7mmHg(p
=00
1).Seven
ofthem
presentedLE
SPof
<12mmHgandtenpatientspresented
LESP
of<6
mmHgaftertheop
eration.
Furtherm
ore,the
abdo
minallength
andtotallengthof
thehigh
pressure
zone
attheesop
hagogastricjunction
wereaffected.
Asleeve
gastrectom
yprod
uces
anim
portantd
ecreasein
LES
pressure,w
hich
can,
inturn,cause
theappearance
ofreflux
symptom
sandesop
hagitisaftertheop
erationdu
eto
apartial
resectionof
theslingfibersdu
ring
thegastrectom
y.
7Gastroenterology Research and Practice

Table2:Stud
iesassessingstom
achmotility.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
1Vives,M
.etal.,
2017
[14],Spain
Prospective
rand
omized
stud
y
60(30patientswiththe
sectionat3cm
and30
patients
withthat
at8cm
from
thepylorus
Gastricem
ptying
byscintigraphy
(T1/2min),gastricvolumeby
CT
scan
(cc)
at6and12
mon
ths
38F/3cm
/8cm
Gastricem
ptying
increasesthespeedsignificantly
inboth
grou
psbu
tisgreaterin
the3cm
grou
p(p
<0 0
5).
Whendividing
grou
psinto
type
2diabeticpatients
andno
ndiabeticpatients,the
speedin
nond
iabetic
patientsissignificantlyhigher
forthe3cm
grou
p.The
residu
alvolumeincreasessignificantlyin
both
grou
ps,and
thereareno
differencesbetweenthem
.Gastricem
ptying
isfaster
inpatientswithantrum
resection.
The
distance
does
notinfluencethegastric
emptying
ofdiabeticpatients.
2Berry,R
.etal.,
2017
[28],
New
Zealand
Prospective
stud
y8(1
patientwithchronic
refux,nausea,and
dysm
otility)
Laparoscop
ichigh-resolution
(HR)electricalmapping
before
andafterLSG
NR
The
baselin
eactivity
show
edexclusivelyno
rmal
prop
agation.
AcutelyafterLSG,allpatients
developedeither
adistalun
ifocalectop
icpacemaker
withretrograde
prop
agation(50%
)or
bioelectricalq
uiescence(50%
).The
prop
agation
velocitywas
abno
rmallyrapidafterLSG(12.5±0.8
versus
baselin
e3.8±0.8mms−
1 ;p=00
1),w
hereas
thefrequencyandam
plitud
ewereun
changed
(2.7±0
.3versus
2.8±0.3cpm,p
=0 7
;1.7±0.2
versus
1.6±0.6mV,p
=0 7
).In
thepatientwith
chronicdysm
otility
afterLSG,m
apping
also
revealed
astableantralectopicpacemaker
with
retrograde
rapidprop
agation(12.6±4.8mms−
1 ).
The
resectionof
thegastricpacemaker
during
LSG
acutelyresultedin
aberrant
distalectopic
pacemakingor
bioelectricalq
uiescence.
Ectop
icpacemakingcanpersistlong
afterLSG,
indu
cing
chronicdysm
otility.
The
clinicalandtherapeuticsignificanceof
these
find
ings
nowrequ
irefurtherinvestigation.
3Sista,F.
etal.,
2017
[16],Italy
Prospective
stud
y52
Gastricem
ptying
scintigraphy
for
liquidandsolid
food
s,before
and
3mon
thsafterLSG.
36F/5cm
After
surgery,T1/2was
significantlyaccelerated:
15.2±13
min
and33.5±18
min
intheLgrou
pand
Sgrou
p,respectively(p
<05).In
both
grou
ps,
GLP
-1plasmaconcentrations
wereincreasedat
each
bloodsamplingtime:2.91
±2.9pg/m
L,3.06
±3.1pg/m
L,and3.21
±2.6pg/m
Lat
15,30,
and60
minutes,respectively,(p
<05)fortheL
grou
pand2.72
±1.5pg/m
L,2.89
±2.1pg/m
L,2.93
±1.8pg/m
L,and2.95
±1.9pg/m
Lat
30,60,
8 Gastroenterology Research and Practice

Table2:Con
tinu
ed.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
90,and
120minutes,respectively,(p
<05)forthe
Sgrou
p.After
LSG,G
LP-1
and%GRpresenteda
negative
linearcorrelation(r)at
each
blood
samplingtimein
both
grou
ps.R
apid
gastric
emptying
3mon
thsafterLSG
4Vigneshwaran,B
.etal.,2016
[26],
India
Prospective
stud
y20
withT2D
Mandwitha
BMIof
30.0–35.0kg/m
2
The
gastricem
ptying
times
were
measuredatbaselin
e,3mon
ths,6
mon
ths,12
mon
ths,and24
mon
thsaftersurgery.
36F/4cm
There
was
asignificant
decrease
ingastric
emptying
time.
Accelerated
gastricem
ptying
5Mans,E.etal.,
2015
[15],Spain
Prospective
comparative
stud
y
Three
grou
pswerestud
ied:
morbidlyobesepatients
(n=16),morbidlyobese
patientswho
hadhadsleeve
gastrectom
y(n
=8),and
nono
bese
patients(n
=16)
Gastricandgallbladd
erem
ptying
42F/5cm
The
antrum
area
during
fastingin
morbidlyobese
patientswas
statistically
significantlylarger
than
that
intheno
nobese
andsleeve
gastrectom
ygrou
ps.G
astricem
ptying
was
acceleratedin
the
sleeve
gastrectom
ygrou
pcomparedwiththeother
2grou
ps(w
hich
hadvery
similarresults).
Gallbladd
erem
ptying
was
similarin
the3grou
ps.
Gastricem
ptying
was
acceleratedin
thesleeve
gastrectom
ygrou
pcomparedwiththeother2
grou
ps(w
hich
hadvery
similarresults)
6Kandeel,A
.A.etal.,
2015
[29],E
gypt
Prospective
stud
y40
Tc-sulfu
rcolloid
GEscintigraphy
was
performed
onallp
atients
subm
ittedto
LSGbeforeandafter
surgery(1–4
weeks
forliq
uids
and4–6weeks
forsolid
s)
36F/3–4cm
T1/2was
significantlyenhanced
afterLSG
comparedwiththebaselin
e(25.3±4.4versus
11.8±3.0min
forliq
uids
and74.9±7.1versus
28.4±8.3min
forsolid
s,resp.,p<0 0
01).The
percentage
ofgastricretentionin
operated
patients
was
significantlylessthan
that
atbaselin
efor
liquids
at15,30,and60
min
(33.9±5.6,17.7±3.9,
and7.5±2.8%
versus
69.4±10.5,55.6±14.95,and
26.1±4.7%
,resp.,p
<0001),aswellasforsolid
sat
30,60,90,and
120min
(42.0±11.1,20.8±6.1,
11.0±5.9,and3.8±2.7%
versus
79.9±8.7,
67.4±12.2,37.0±10.9%,and
13.8±4.4%
,resp.,
p<0 0
01).
The
significant
acceleration
ofGEof
liquids
and
solid
safterLSGmay
have
contribu
tedto
weight
lossin
theim
mediatepo
stop
erativeperiod
(4–6
weeks).
Itremains
tobe
determ
ined
whether
theweight
losswill
continue
beyond
that
period
.
9Gastroenterology Research and Practice

Table2:Con
tinu
ed.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
7Burgerhart,J.S.
etal.,2015
[24],
Netherlands
Prospective
stud
y20
Gastricem
ptying
stud
ywithsolid
andliq
uidmealcom
ponentsin
thesecond
year
afterLSG
34F/6cm
The
lagph
ase(solid)was
6.4±4.5min
ingrou
pI
and7.3±6.3ingrou
pII(p
=09
4);T
1/2(solid)w
as40.6±10.0miningrou
pIand
34.4±9.3ingrou
pII
(p=0 2
7);the
caloricem
ptying
ratewas
3.9
±0.6kcal/m
inin
grou
pIand3.9±1.0kcal/m
inin
grou
pII(p
=0 3
2).
Patientswithpo
stprandialsymptom
safterLSG
repo
rted
moresymptom
sdu
ring
thegastric
emptying
stud
ythan
didpatientswitho
utsymptom
s.How
ever,there
was
nodifference
betweengastricem
ptying
characteristicsbetween
both
grou
ps,suggestingthat
abno
rmalgastric
emptying
isno
tamajor
determ
inantof
postprandialsymptom
safterLSG.
8Melissas,J.etal.,
2013
[21],G
reece
Prospective
stud
y21
The
gastrictransittimes
were
stud
iedwithagammacamera
before
and4mon
ths
postop
eratively
34F/5cm
SGacceleratesthegastricem
ptying
ofsemisolids
9Pilo
ne,V
.etal.,
2013
[17],Italy
Prospective
controlled
rand
omized
stud
y
45Group
Aexam
before
(A1)
andaftertheop
eration(A
2).
Con
trol
grou
p(G
roup
B)
Gastricem
ptying
scintigraphy
1mon
thpreoperativelyand3
mon
thspo
stop
eratively
34Ch/4–5cm
The
scintigraphicstud
yshow
edaredu
cedhalf-life
tracer
(A1versus
A2:80.4±16.5min
versus
64.3±22
min
p=0 0
6),w
itho
utasignificant
difference.C
omparing
thetwogrou
ps,n
odifferencesoccurred
before
operation(B
versus
A1).T
hegastricem
ptying
timeresulted
ina
significant
redu
ctionin
grou
pA2rather
than
ingrou
psA1andB.
LSGredu
cesgastricem
ptying
time
10Michalsky,D
.etal.,
2013
[22],
Czech
Repub
lic
Prospective
rand
omized
stud
y12
Group
Aantrum
resection
Group
BAntrum
preservation
Gastricem
ptying
scintigraphy
before
and3mon
ths
postop
eratively
42F/7cm
Intheantrum
resectiongrou
p,theaveragetime
T1/2declined
from
57.5to
32.25min
(p=0 0
16)
andaverageretention%GEdrop
pedfrom
20.5to
9.5%
(p=0 0
73).
Intheantrum
resectiongrou
p,an
increase
ingastricem
ptying
postop
erativelywas
noted.
Com
plications
such
asfailu
reof
stom
ach
evacuation
wereno
tobserved
intheRAgrou
p;even
moreradicalresection
ofthepyloricantrum
performed
byLSGispo
ssiblewitho
utconcerns
ofpo
stop
erativedisorder
ofthestom
achevacuation
function
10 Gastroenterology Research and Practice

Table2:Con
tinu
ed.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
11Parikh,
M.etal.,
2012
[25],U
SA
Datafrom
aninstitutional
review
board-
approved
electron
icregistry
62
Gastrod
uodenaltransittime
(antrum
todu
odenum
)was
calculated
from
apo
stop
erative
day1esop
hagram
.Postoperative
esop
hagram
s
40F/5–7cm
The
meangastrodu
odenaltransittimewas
12.3±19.8s.Alm
ostallp
atients(99%
)hada
transittimeof
lessthan
60s.
Nocorrelationwas
foun
dbetweengastrodu
odenal
transittimeand%EWLat
3,6,or
12mon
ths.
12Baumann,
T.etal.,
2011
[23],G
ermany
Prospective
pilot
stud
y5
MRI1daybefore
LSGand6days
and6mon
thsafterLSG
32F/5–6cm
The
dynamicanalysisshow
edthat
antral
prop
ulsive
peristalsiswas
preservedim
mediately
aftersurgeryanddu
ring
follow-up,
butfold
speed
increasedsignificantlyfrom
2.7mm/sbefore
LSG
to4.4mm/safter6mon
ths.The
sleeve
itself
remainedwitho
utrecognizableperistalsisin
three
patientsandshow
edon
lyun
coordinatedor
passive
motionin
twopatients.C
onsequ
ently,thefluid
transportthrou
ghthesleeve
was
markedlydelayed,
whereastheantrum
show
edacceleratedprop
ulsion
withtheem
ptying
half-timedecreasing
from
16.5min
preoperativelyto
7.9min
6mon
thsafter
surgery.
The
stom
achisfunction
allydividedinto
asleeve
witho
utprop
ulsive
peristalsisandan
accelerated
antrum
.Accelerated
emptying
seem
sto
becaused
byfaster
peristalticfolds.
13Pom
erri,F
.etal.,
2011
[18],Italy
Retrospective
stud
y57
The
size
ofthegastricfund
usremaining
afterLSGandgastric
voidingrate(fast/slow
)by
radiologicalup
per
gastrointestinalseries
(UGS)
with
awater-solub
lecontrastmedium
(CM).
NR/4–6
cm
Sleeve
voidingwas
fastin
49of
57patients
(85.96%)andslow
ineight(14.03%).
Patientsshow
ingarapidgastrodu
odenaltransitof
theCM
achieved
abetter
weightlossthan
patients
withaslow
voidingrate.
14Shah,S.etal.,
2010
[27],Ind
iaProspective
controlledstud
y
24werelean
controls(bod
ymassindex22.2±2.84
kg/m
(2)),20wereseverelyand
morbidlyobesepatientswith
T2D
Mwho
hadno
tun
dergon
eSG
(bod
ymass
index37.73±5.35
kg/m
(2)),
and23
wereseverelyand
morbidlyobesepatientswith
T2D
MafterSG
.
Scintigraphicim
agingwith
g-camera
NR
The
gastricem
ptying
half-timevalues
werealso
significantlyshorter(p
<05)in
thepo
st-SG
(52.8±13.5minutes)than
intheno
n-SG
(73.7±29.0minutes)andcontrol(72.8±29.6
minutes)grou
psdecreasedgastricem
ptying
half-timeafterSG
11Gastroenterology Research and Practice

Table2:Con
tinu
ed.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
15Braghetto,I.etal.,
2009
[30],C
hile
Prospective
stud
y20
obesesubm
ittedto
LSG
18no
rmalsubjects
Gastricem
ptying
ofliq
uids
and
solid
swas
measuredby
scintigraphictechniqu
e3mon
ths
postop
eratively.
32F/2cm
Inthegrou
pof
operated
patients,70%
ofthem
(n=14)presentedacceleratedem
ptying
forliq
uids
and75%(n
=15)forsolid
scomparedto
22.2%and
27.7%,respectively,in
thecontrolgroup
.The
half-timeof
gastricem
ptying
(T(1/2))in
patients
subm
ittedto
SGboth
forliq
uids
andsolid
swere
significantlymoreacceleratedcomparedto
the
controlgroup
(34.9±24.6versus
13.6±11.9min
forliq
uids
and78
±15.01versus
38.3±18.77min
forsolid
s;p<0 0
1).T
hegastricem
ptying
for
liquids
expressedas
thepercentagesof
retentionat
20,30,and60
min
were30.0±0.25%,15.4±0.18%,
and5.7±0.10%,respectively,in
operated
patients,
significantlylessthan
thecontrolsub
jects
(p<0 0
01).Fo
rsolid
s,thepercentage
ofretention
at60,90,and120minwas56
+/−
28%,34+/−
22%,
and12
+/−
8%,respectively,forcontrols,w
hileit
was
25.3+/−
0.20%,9
+/−
0.12%,and
3+/−
0.05%,
respectively,inop
erated
patients(p
<001).
Gastricem
ptying
afterSG
isacceleratedeither
forliq
uids
aswellasforsolid
sin
themajority
ofpatients.
16Bernstine
Hetal.,
2009
[31],Israel
Prospective
stud
y21
Gastricem
ptying
scintigraphy
ofsemisolidswas
performed
before
and3mon
thsafterLSG
48F/6cm
The
meanT1/2rawdata
were62.39±19.83and
56.79±18.72min
(p=036,t
=−0
92,N
S)before
and3mon
thsafterLSG,respectively.The
T1/2
linearwas
103.64
±9.82
and106.92
±14.55,
(p=0 4
3,t=
−043,N
S),and
thelin
earfitslop
e0.48
±0.04
and0.47
±0.05
(p=0 4
8,t=
07,N
S).
LSGwithantrum
preservation
asperformed
inthis
series
hasno
effecton
gastricem
ptying.
17Melissas,J.etal.,
2008
[20],G
reece
Prospective
stud
y14
Ninepatientsun
derw
entgastric
emptying
stud
ies,using
radioisotopictechniqu
ebefore,6
mon
ths,and24
mon
thsafterthe
operation.
The
remaining
five
patientsun
derw
entgastric
emptying
stud
ies,6mon
thsand
24mon
thsaftertheop
eration.
Scintigraphicim
agingwas
performed
withaγ-camera
NR
Inthenine
patientswho
underw
entgastric
emptying
stud
iespreoperativelyand6and24
mon
thspo
stop
eratively,theT-lag
phasedu
ration
significantlydecreased,
followingtheSG
,from
17.30(range
15.50–20.90)
min,to12.50(range
9.20–18.00)min
at6mon
thsand12.16(range
10.90–20.00)
min
at24
mon
thspo
stop
eratively
(p<005)
The
gastricem
ptying
halftime(T1/2)
accelerated
significantlypo
stop
erativelyfrom
86.50(range
77.50–104.60)min,to62.50(range
46.30–80.00)
12 Gastroenterology Research and Practice

Table2:Con
tinu
ed.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment/
follow-uppo
ints
Bou
giesize/distance
from
pylorus
Mainfind
ings
ofthestud
y
min
at6mon
thsand60.80(range
54.80–100.00)
min
at24
mon
thsafterSG
(p<0 0
5).T
hepercentage
ofgastricem
ptying
(%GE)increased
significantlypo
stop
eratively,from
52(range
43–58)
%to
72(range
57–97)
%at
6mon
thsand
74(range
45–82)
%at
24mon
ths,followingSG
(P<0 0
5).N
odifferencesin
gastricem
ptying
were
observed,w
henvalues
at24
mon
thswere
comparedto
thoseat
6mon
thspo
stop
eratively.
Whenthewho
legrou
pof
14patientswas
stud
ied,
therewerealso
nosignificant
changesin
T-lag,
T1/2and%GEbetween6and24
mon
ths
postop
eratively.
Con
stanteffectof
SGin
theacceleration
ofgastric
emptying
ofsolid
s,which
occursfaster,not
onlyin
shortbu
talso
inlong-term
postop
eratively
18Melissas,J.etal.,
2007
[19],G
reece
Prospective
stud
y23
The
scintigraphicmeasurement
ofthegastricem
ptying
ofasolid
mealp
reop
erativelyand6
mon
thspo
stop
eratively.
Gastricem
ptying
stud
iesusing
radioisotopictechniqu
ebefore
and6mon
thsaftertheop
eration.
34F/7cm
Alth
ough
themealsizewas
drastically
redu
ced,the
mealfrequ
ency
increasedpo
stop
erativelyin
12patients(52.2%
).Only5patients(21.8%
)repo
rted
occasion
alvomitingaftermealsfollowingSG
.The
gastric
emptying
half-time(T1/2)
accelerated(47.6±23.2
versus
94.3±15.4,p
<0 0
1),and
theT-lag
phase
duration
decreased(9.5±2
min
versus
19.2±2min,p
<005)po
stop
eratively.The
percentage
ofthemealemptiedfrom
thestom
ach
90min
afterconsum
ptionincreasedsignificantly
afterSG
(75.4±14.9%
versus
49.2±8.7%
,p<001);thestom
achem
ptiesitscontentsrapidly
into
thesm
allintestine
andsymptom
sof
vomiting
aftereating
(characteristicof
restrictive
procedures)areeither
absent
orvery
mild
NR:n
otrepo
rted.
13Gastroenterology Research and Practice

Table3:Stud
iesassessingbowelmotility.
Autho
r,year
ofpu
blication,
coun
try
Typeof
stud
yPatients(N
)Metho
dof
assessment
Stud
ymainfind
ing
1Trung,V
.N.etal.,
2013
[32],Japan
Prospective
stud
y12
Intestinalmotility
during
OGTTwas
assessed
usingcine
MRIbefore
and3mon
ths
postop
eratively
LSGleadsto
acceleratedintestinalmotility
and
redu
cedintestinaltransittime
2Melissas,J.etal.,
2013
[21],G
reece
Prospective
stud
y21
g-Cam
erabefore
and4mon
thspo
stop
eratively
LSGacceleratesthesm
allb
oweltransitof
semisolids.In
addition
,itdelays
theinitiation
ofcecalfi
lling
andTICVt.
3Shah,S.etal.,
2010
[27],Ind
iaProspective
controlledstud
y
67Con
trols:24
MorbidlyobesepatientswithT2D
Mno
tun
dergon
eSG
:20
MorbidlyobesepatientswithT2D
MafterSG
:23
Scintigraphicim
aging
Decreased
smallb
oweltransittimeafterSG
14 Gastroenterology Research and Practice

of the normal gastric pacemaker during LSG had as a resultthe acute gastric slow-wave quiescence or the generation ofdistal ectopic pacemakers accompanied by a markedlyincreased propagation velocity. It seems that the sleeve affectsthe electrophysiology of the stomach. Further studies areneeded to support this.
There was a consensus except for one study that gastricemptying was accelerated. The rapid gastric emptying wasalso strengthened by the observation of our team that asignificant proportion of patients experienced dumpingsyndrome upon provocation at six weeks and 6 and 12months after LSG. These symptoms included both earlyand late symptoms suggesting that LSG may lead tochanges in eating patterns after LSG, especially in sweeters[37, 38]. Only one study showed no effect on gastricemptying. In this study, the follow-up was done in 3months, and the created sleeve was performed using abougie 48F at a distance of 6 cm from the pylorus [31].Therefore, the sleeve might be large enough withoutincreasing its intraluminal pressure.
There is still a debate concerning the maintenance ofthe antrum in order to avoid interference with the gastricphysiology or its resection to increase the restrictive mech-anism. Abdallah et al., who compared groups with resec-tions at 2 cm versus 6 cm distances from the pylorus,showed that there was statistically significant excess weightloss between the groups, concluding that increasing the sizeof the resected antrum was associated with better weightloss, without increasing significantly the rate of complica-tions [39]. Similarly, Obeidat et al. showed that patientswith resection at 2 cm distance from the pylorus experi-enced statistically significant better maintained weight lossthan did patients with resection at 6 cm [40]. On the con-trary, ElGeidie et al. found no statistical differences regard-ing weight loss at the groups at 2 cm and 6 cm from thepylorus [41]. Vives et al. showed that gastric emptyingwas faster in the group with the resection at 3 cm fromthe pylorus compared to that at 8 cm from the pylorus at6 and 12 months postoperatively [14]. Unlike the previous,Fallahat et al. compared the gastric emptying in patients at4 cm and 7 cm distance from pylorus 3 months postopera-tively. The authors showed that resection at 4 cm fromthe pylorus were associated with delayed gastric emptying,and resection at 7 cm from the pylorus, with acceleratedgastric emptying. The authors speculated that resection at4 cm from the pylorus had as a consequence neural inner-vations of the antrum being abolished, contributing toslower emptying. These patients experienced nausea, vomit-ing, and poor appetite. On the other hand, the resectionat 7 cm from the pylorus preserved the contractility ofthe antrum, leading to rapid gastric emptying due to theabsence of redistribution process since the body and funduswere excised. These patients complained of dumping-likesymptoms and had more frequent meals [42]. Furtherprospective randomized trials are needed to compare themotility changes and clinical symptoms in patients with thepreservation or not of antrum.
There is scant information concerning the possibleexplanation of how these motility alterations may affect
clinical symptoms or explain the underlying mechanisms ofaction. It seems that the technique is not standardized, anddifferent sleeves are created. Thus, different residual gastricvolumes are produced. Since now, no clear association wasfound between gastric volume and weight loss. Researcherssuggest that the physiological changes and not the size ofthe sleeve are responsible as mechanisms of action. What isknown is that LSG changes the profile of gut hormones. Sistaet al. showed that the rapid gastric emptying was correlatedwith the increased production of GLP-1 in the distal bowel[16]. Burgerhart et al. associated postprandial symptomswith gastric emptying. No difference on gastric-emptyingcharacteristics was found between patients with low orhigh postprandial symptoms [24]. Pomerri et al. foundthat patients presenting with a rapid gastroduodenal transitexperienced better weight loss than patients presenting witha slow voiding rate [18]. It seems that little is known regard-ing the underlining mechanisms by which LSG controlsappetite and food intake. Since the data are restricted tomedium term, it would be interesting to see if the sleevebehaves differently in the long term and how weight regainis explained in some patients.
Bowel motility was the least studied. It seems that thefood reaches the terminal ileum faster but arrives at thececum later. Thus, the contact of the food with the area of ter-minal ileum is extended. Perhaps, this altered interaction offood with the gastrointestinal tract may be a key componentto explain the neurohormonal changes via the stimulation ofintestinal L cells producing incretions and understandingthe underlining mechanisms which improve the metabolicprofile of the patients.
The limitations of the review include the lack ofstandardization of the surgical technique, the differentfollow-up timings, the different measured outcomes, thesmall sample siz,e and the lack of available long-term databeyond four years.
Further pathophysiological studies are needed to inves-tigate the exact correlation of the motility parameters withthe clinical symptoms and gut peptide alterations andpotential hormonal interactions between gastrointestinaltract and brain.
5. Conclusion
Laparoscopic sleeve gastrectomy has impacts on the gastro-intestinal motility. The data remain debatable for esophagealmotility. The stomach and small bowel motilities wereaccelerated, while the initiation of cecal filling and theileocecal valve transit was delayed. Further pathophysiologi-cal studies are needed to investigate the exact correlation ofthe motility parameters with the clinical symptoms and gutpeptide alterations.
Conflicts of Interest
The authors declare that there is no conflict of interestregarding the publication of this article.
15Gastroenterology Research and Practice

References
[1] L. Angrisani, A. Santonicola, P. Iovino et al., “Bariatric surgeryand endoluminal procedures: IFSO worldwide survey 2014,”Obesity Surgery, vol. 27, no. 9, pp. 2279–2289, 2017.
[2] M. M. Hutter, B. D. Schirmer, D. B. Jones et al., “First reportfrom the American College of Surgeons Bariatric Surgery Cen-ter Network: laparoscopic sleeve gastrectomy has morbidityand effectiveness positioned between the band and thebypass,” Annals of Surgery, vol. 254, no. 3, pp. 410–422, 2011.
[3] S. H. Chang, C. R. Stoll, J. Song, J. E. Varela, C. J. Eagon, andG. A. Colditz, “The effectiveness and risks of bariatric surgery:an updated systematic review and meta-analysis, 2003-2012,”JAMA Surgery, vol. 149, no. 3, pp. 275–287, 2014.
[4] R. T. Yehoshua, L. A. Eidelman, M. Stein et al., “Laparoscopicsleeve gastrectomy—volume and pressure assessment,” Obe-sity Surgery, vol. 18, no. 9, pp. 1083–1088, 2008.
[5] E. Sioka, G. Tzovaras, F. Tsiopoulos et al., “Esophageal motilityafter laparoscopic sleeve gastrectomy,” Clinical and Experi-mental Gastroenterology, vol. 10, pp. 187–194, 2017.
[6] E. Kleidi, D. Theodorou, K. Albanopoulos et al., “The effect oflaparoscopic sleeve gastrectomy on the antireflux mechanism:can it be minimized?,” Surgical Endoscopy, vol. 27, no. 12,pp. 4625–4630, 2013.
[7] F. Mion, S. Tolone, A. Garros et al., “High-resolutionimpedance manometry after sleeve gastrectomy: increasedintragastric pressure and reflux are frequent events,” ObesitySurgery, vol. 26, no. 10, pp. 2449–2456, 2016.
[8] F. Rebecchi, M. E. Allaix, C. Giaccone, E. Ugliono, G. Scozzari,and M. Morino, “Gastroesophageal reflux disease and laparo-scopic sleeve gastrectomy: a physiopathologic evaluation,”Annals of Surgery, vol. 260, no. 5, pp. 909–915, 2014.
[9] G. Del Genio, S. Tolone, P. Limongelli et al., “Sleeve gastrec-tomy and development of “de novo” gastroesophageal reflux,”Obesity Surgery, vol. 24, no. 1, pp. 71–77, 2014.
[10] V. Gorodner, R. Buxhoeveden, G. Clemente, L. Solé, L. Caro,and A. Grigaites, “Does laparoscopic sleeve gastrectomy haveany influence on gastroesophageal reflux disease? Prelimi-nary results,” Surgical Endoscopy, vol. 29, no. 7, pp. 1760–1768, 2015.
[11] J. S. Burgerhart, C. A. Schotborgh, E. J. Schoon et al.,“Effect of sleeve gastrectomy on gastroesophageal reflux,”Obesity Surgery, vol. 24, no. 9, pp. 1436–1441, 2014.
[12] W. V. Petersen, T. Meile, M. A. Küper, M. Zdichavsky,A. Königsrainer, and J. H. Schneider, “Functional importanceof laparoscopic sleeve gastrectomy for the lower esophagealsphincter in patients with morbid obesity,” Obesity Surgery,vol. 22, no. 3, pp. 360–366, 2012.
[13] I. Braghetto, E. Lanzarini, O. Korn, H. Valladares, J. C. Molina,and A. Henriquez, “Manometric changes of the loweresophageal sphincter after sleeve gastrectomy in obesepatients,” Obesity Surgery, vol. 20, no. 3, pp. 357–362, 2010.
[14] M. Vives, A. Molina, M. Danús et al., “Analysis of gastricphysiology after laparoscopic sleeve gastrectomy (LSG) withor without antral preservation in relation to metabolicresponse: a randomised study,” Obesity Surgery, vol. 27,no. 11, pp. 2836–2844, 2017.
[15] E. Mans, M. Serra-Prat, E. Palomera, X. Suñol, and P. Clavé,“Sleeve gastrectomy effects on hunger, satiation, and gastroin-testinal hormone and motility responses after a liquid mealtest,” The American Journal of Clinical Nutrition, vol. 102,no. 3, pp. 540–547, 2015.
[16] F. Sista, V. Abruzzese, M. Clementi, S. Carandina, M. Cecilia,and G. Amicucci, “The effect of sleeve gastrectomy on GLP-1secretion and gastric emptying: a prospective study,” Surgeryfor Obesity and Related Diseases, vol. 13, no. 1, pp. 7–14, 2017.
[17] V. Pilone, S. Tramontano, R. Di Micco et al., “Gastric empty-ing after sleeve gastrectomy: statistical evidence of a controlledprospective study with gastric scintigraphy,” Minerva Chirur-gica, vol. 68, no. 4, pp. 385–392, 2013.
[18] F. Pomerri, M. Foletto, G. Allegro, P. Bernante, L. Prevedello,and P. C. Muzzio, “Laparoscopic sleeve gastrectomy–radiological assessment of fundus size and sleeve voiding,”Obesity Surgery, vol. 21, no. 7, pp. 858–863, 2011.
[19] J. Melissas, S. Koukouraki, J. Askoxylakis et al., “Sleeve gastrec-tomy: a restrictive procedure?,” Obesity Surgery, vol. 17, no. 1,pp. 57–62, 2007.
[20] J. Melissas, M. Daskalakis, S. Koukouraki et al., “Sleevegastrectomy-a “food limiting” operation,” Obesity Surgery,vol. 18, no. 10, pp. 1251–1256, 2008.
[21] J. Melissas, A. Leventi, I. Klinaki et al., “Alterations of globalgastrointestinal motility after sleeve gastrectomy: a prospectivestudy,” Annals of Surgery, vol. 258, no. 6, pp. 976–982, 2013.
[22] D. Michalsky, P. Dvorak, J. Belacek, and M. Kasalicky,“Radical resection of the pyloric antrum and its effect ongastric emptying after sleeve gastrectomy,” Obesity Surgery,vol. 23, no. 4, pp. 567–573, 2013.
[23] T. Baumann, S. Kuesters, J. Grueneberger et al., “Time-resolvedMRI after ingestion of liquids reveals motility changesafter laparoscopic sleeve gastrectomy–preliminary results,”Obesity Surgery, vol. 21, no. 1, pp. 95–101, 2011.
[24] J. S. Burgerhart, P. W. van Rutte, M. A. Edelbroek et al.,“Association between postprandial symptoms and gastricemptying after sleeve gastrectomy,” Obesity Surgery, vol. 25,no. 2, pp. 209–214, 2015.
[25] M. Parikh, J. Eisner, N. Hindman, E. Balthazar, and J. K.Saunders, “Tests of correlation between immediate postopera-tive gastroduodenal transit times and weight loss after laparo-scopic sleeve gastrectomy,” Surgical Endoscopy, vol. 26, no. 12,pp. 3548–3551, 2012.
[26] B. Vigneshwaran, A. Wahal, S. Aggarwal et al., “Impact ofsleeve gastrectomy on type 2 diabetes mellitus, gastric empty-ing time, glucagon-like peptide 1 (GLP-1), ghrelin and leptinin non-morbidly obese subjects with BMI 30-35.0 kg/m2: aprospective study,” Obesity Surgery, vol. 26, no. 12, pp. 2817–2823, 2016.
[27] S. Shah, P. Shah, J. Todkar, M. Gagner, S. Sonar, and S. Solav,“Prospective controlled study of effect of laparoscopic sleevegastrectomy on small bowel transit time and gastric emptyinghalf-time in morbidly obese patients with type 2 diabetesmellitus,” Surgery for Obesity and Related Diseases, vol. 6,no. 2, pp. 152–157, 2010.
[28] R. Berry, L. K. Cheng, P. Du et al., “Patterns of abnormalgastric pacemaking after sleeve gastrectomy defined bylaparoscopic high-resolution electrical mapping,” ObesitySurgery, vol. 27, no. 8, pp. 1929–1937, 2017.
[29] A. A. Kandeel, M. D. Sarhan, T. Hegazy, M. M. Mahmoud, andM. H. Ali, “Comparative assessment of gastric emptying inobese patients before and after laparoscopic sleeve gastrectomyusing radionuclide scintigraphy,” Nuclear Medicine Commu-nications, vol. 36, no. 8, pp. 854–862, 2015.
[30] I. Braghetto, C. Davanzo, O. Korn et al., “Scintigraphic evalu-ation of gastric emptying in obese patients submitted to sleeve
16 Gastroenterology Research and Practice

gastrectomy compared to normal subjects,” Obesity Surgery,vol. 19, no. 11, pp. 1515–1521, 2009.
[31] H. Bernstine, R. Tzioni-Yehoshua, D. Groshar et al., “Gastricemptying is not affected by sleeve gastrectomy–scintigraphicevaluation of gastric emptying after sleeve gastrectomy with-out removal of the gastric antrum,” Obesity Surgery, vol. 19,no. 3, pp. 293–298, 2009.
[32] V. N. Trung, H. Yamamoto, A. Furukawa et al., “Enhancedintestinal motility during oral glucose tolerance test afterlaparoscopic sleeve gastrectomy: preliminary results using cinemagnetic resonance imaging,” PLoS One, vol. 8, no. 6, articlee65739, 2013.
[33] M. Gagner, M. Deitel, T. L. Kalberer, A. L. Erickson, and R. D.Crosby, “The Second International Consensus Summit forSleeve Gastrectomy, March 19-21, 2009,” Surgery for Obesityand Related Diseases, vol. 5, no. 4, pp. 476–485, 2009.
[34] P. Prinz and A. Stengel, “Control of food intake by gastrointes-tinal peptides: mechanisms of action and possible modulationin the treatment of obesity,” Journal of Neurogastroenterologyand Motility, vol. 23, no. 2, pp. 180–196, 2017.
[35] A. Inui, A. Asakawa, C. Y. Bowers et al., “Ghrelin, appetite, andgastric motility: the emerging role of the stomach as anendocrine organ,” The FASEB Journal, vol. 18, no. 3,pp. 439–456, 2004.
[36] P. Janssen, P. Vanden Berghe, S. Verschueren, A. Lehmann,I. Depoortere, and J. Tack, “Review article: the role of gastricmotility in the control of food intake,” Alimentary Pharmacol-ogy & Therapeutics, vol. 33, no. 8, pp. 880–894, 2011.
[37] G. Tzovaras, D. Papamargaritis, E. Sioka et al., “Symptomssuggestive of dumping syndrome after provocation in patientsafter laparoscopic sleeve gastrectomy,”Obesity Surgery, vol. 22,no. 1, pp. 23–28, 2012.
[38] D. Papamargaritis, G. Koukoulis, E. Sioka et al., “Dumpingsymptoms and incidence of hypoglycaemia after provocationtest at 6 and 12 months after laparoscopic sleeve gastrectomy,”Obesity Surgery, vol. 22, no. 10, pp. 1600–1606, 2012.
[39] E. Abdallah, A. El Nakeeb, T. Youssef et al., “Impact of extentof antral resection on surgical outcomes of sleeve gastrectomyfor morbid obesity (a prospective randomized study),” ObesitySurgery, vol. 24, no. 10, pp. 1587–1594, 2014, Erratum in: ObesSurg. 2015 Oct;25(10):1987. Yousef, Tamer [Corrected toYoussef, Tamer].
[40] F. Obeidat, H. Shanti, A. Mismar, N. Albsoul, andM. Al-Qudah, “The magnitude of antral resection in laparo-scopic sleeve gastrectomy and its relationship to excess weightloss,” Obesity Surgery, vol. 25, no. 10, pp. 1928–1932, 2015.
[41] A. ElGeidie, M. ElHemaly, E. Hamdy, M. El Sorogy,M. AbdelGawad, and N. GadElHak, “The effect of residualgastric antrum size on the outcome of laparoscopic sleeve gas-trectomy: a prospective randomized trial,” Surgery for Obesityand Related Diseases, vol. 11, no. 5, pp. 997–1003, 2015.
[42] B. Fallatah, A. AzizShehry, L. Abdelsamad, H. Zaid,S. Hussain, and S. Jaber, “Comparison study of gastric empty-ing after performing sleeve gastrectomy with two differenttechniques,” Journal of Surgery, vol. 1, no. 4, pp. 53–56, 2013.
17Gastroenterology Research and Practice

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com



![PneuSleeve: In-fabric Multimodal Actuation and Sensing in a Soft, … · 2020-04-16 · Zhu, 2020 (this work) sleeve pneumatic tube in fabric cap. X X X Pezent [17], 2019 bracelet](https://static.fdocuments.ec/doc/165x107/5fb1d6a733830c6aa8025b90/pneusleeve-in-fabric-multimodal-actuation-and-sensing-in-a-soft-2020-04-16-zhu.jpg)













