Hepatitis B virus combo mutations improve the prediction and … · 2015. 8. 19. · We aimed to...
45
1 Hepatitis B virus combo mutations improve the prediction and active prophylaxis of hepatocellular carcinoma: a clinic-based cohort study Running title: Prediction and prophylaxis of HCC and death Jianhua Yin, 1 Junxue Wang, 2 Rui Pu, 1 Haiguang Xin, 2 Zixiong Li, 1 Xue Han, 3 Yibo Ding, 1 Yan Du, 1 Wenbin Liu, 1 Yang Deng, 1 Xiaowei Ji, 1 Ming Wu, 4 Min Yu, 5 Hongwei Zhang, 1 Hongyang Wang, 6 Timothy C. Thompson, 7 Wu Ni, 2 Guangwen Cao 1 1 Department of Epidemiology, Second Military Medical University, Shanghai, China; 2 Department of Infectious Diseases, The 2 nd Affiliated Hospital, Second Military Medical University, Shanghai, China; 3 Division of Chronic Diseases, Center for Disease Control and Prevention of Yangpu District, Shanghai, China; 4 Division of Chronic Diseases, Provincial Center for Disease Control and Prevention of Jiangsu, Nanjing, China; 5 Division of Chronic Diseases, Provincial Center for Disease Control and Prevention of Zhejiang, Hangzhou, China; Cancer Research. on December 7, 2020. © 2015 American Association for cancerpreventionresearch.aacrjournals.org Downloaded from Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160
Transcript of Hepatitis B virus combo mutations improve the prediction and … · 2015. 8. 19. · We aimed to...

1
Hepatitis B virus combo mutations improve the prediction and active
prophylaxis of hepatocellular carcinoma: a clinic-based cohort study
Running title: Prediction and prophylaxis of HCC and death
Jianhua Yin,1 Junxue Wang,2 Rui Pu,1 Haiguang Xin,2 Zixiong Li,1 Xue Han,3 Yibo
Ding,1 Yan Du,1 Wenbin Liu,1 Yang Deng,1 Xiaowei Ji,1 Ming Wu,4 Min Yu,5
Hongwei Zhang,1 Hongyang Wang,6 Timothy C. Thompson,7 Wu Ni,2 Guangwen
Cao1
1 Department of Epidemiology, Second Military Medical University, Shanghai, China;
2 Department of Infectious Diseases, The 2nd Affiliated Hospital, Second Military
Medical University, Shanghai, China;
3 Division of Chronic Diseases, Center for Disease Control and Prevention of Yangpu
District, Shanghai, China;
4 Division of Chronic Diseases, Provincial Center for Disease Control and Prevention
of Jiangsu, Nanjing, China;
5 Division of Chronic Diseases, Provincial Center for Disease Control and Prevention
of Zhejiang, Hangzhou, China;
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

2
6 International Cooperation Laboratory on Signal Transduction, The 3rd Affiliated
Hospital, Second Military Medical University, Shanghai, China;
7 Department of Genitourinary Medical Oncology-Research, University of Texas MD
Anderson Cancer Center, Houston, Texas, USA.
The first 4 authors contributed equally to this work. Guangwen Cao and Wu Ni are
equal senior authors.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed by authors.
Grant support: This study was supported by the National Key Basic Research
Program (2015CB554000 to G. Cao) and Key Project for Infectious Diseases
(2012ZX10002-008 to G. Cao) from the Ministry of Science and Technology of China,
National Natural Science Foundation of China (91129301 to G. Cao, 81025015 to G.
Cao, 81302492 to Y. Du, 81221061 to H. Wang, 81373067 to J. Yin), and Outstanding
Young Investigator Project from Shanghai Municipal Health and Family Planning
Commission (XYQ2013072 to J. Yin).
Corresponding author: Guangwen Cao, Department of Epidemiology, Second
Military Medical University, 800 Xiangyin Road, Shanghai, 200433, People's
Republic of China. Phone: 86-21-81871060; Fax: 86-21-81871060; E-mail:
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

3
Word count: Abstract 250; Main document 3417; References 39; Figures and Tables,
6; Supplementary Tables, 3; Supplementary Figures, 3.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

4
Abstract
We aimed to evaluate if hepatitis B virus (HBV) mutations at the core promoter region
could improve the prediction and specific prophylaxis of hepatocellular carcinoma
(HCC) in chronic HBV-infected patients. A total of 2114 HBV-infected patients
enrolled between August 1998 and December 2007 were followed-up for 18406
person-years. Of those, 612 received ≥48 week treatments with nucleos(t)ide analogue
(NA) and/or interferon-α. Baseline HBV mutations were identified by sequencing.
Propensity score matching was applied to reduce baseline differences between
antiviral and control cohorts. Multivariate Cox regression analyses including baseline
characteristics of 2114 patients showed that age, male, cirrhosis, and HBV mutations
(C1653T, T1753V, and A1762T/G1764A) independently increased HCC risk. In
control patients carrying A1762T/G1764A, addition of C1653T and/or T1753V
significantly increased HCC risk (HR=1.57; P=0.038); combo mutations with C1653T,
T1753V, and A1762T/G1764A improved the validity of HCC prediction by age, male,
and cirrhosis (P=0.002). In the matched cohorts, antiviral treatment reduced HCC
incidence (13.90/1000 vs. 7.70/1000 person-years, P=0.005); NA treatment for ≥60
months was required for the prophylaxis of HCC in cirrhotic patients (P=0.03);
antiviral treatment reduced HCC risk in patients carrying A1762T/G1764A
(HR=0.40; P=0.002) or C1653T (HR=0.45; P=0.04) and in those without T1753V
(HR=0.42; P=0.005), but could not reduce HCC risk in patients without
A1762T/G1764A or C1653T and in those with T1753V. In summary, HBV mutation
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

5
A1762T/G1764A, C1653T, and T1753V in combination improve HCC prediction in
HBV-infected patients. To prevent HCC, patients infected with HBV carrying
A1762T/G1764A or C1653T, but not T1753V, should be given priority of receiving
antiviral treatments.
Keywords: hepatitis B virus; mutation; antiviral treatment; hepatocellular carcinoma;
cohort study
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

6
Introduction
Primary liver cancer is the second leading cause of cancer-related death in men and
the fifth causes of cancer death in women and hepatocellular carcinoma (HCC)
accounts for 70% to 85% of the total liver cancer burden worldwide (1). Chronic
infection with hepatitis B virus (HBV) contributes to more than half of global HCC
cases. The lifetime (30-75 years) incidences of HCC for men and women positive for
hepatitis B surface antigen (HBsAg) were 27.38% and 7.99%, respectively, in Taiwan
(2), an area endemic for HBV genotypes B and C. Therefore, it is estimated that
approximately 20 million HCC cases caused by chronic HBV infection will be
diagnosed in next 50 years in Mainland China, an area with one-third of global
HBV-infected subjects. HCC is a highly fatal malignancy, with a 5-year survival rate
of 9.01% for patients without surgical treatment and 32.64% for those who received
surgery in Shanghai, China (3). Much hope for controlling HCC is placed with active
prophylaxis prior to its occurrence. Fortunately, the occurrence and recurrence of
HBV-related HCC can be reduced via active prophylaxis using anti-HBV treatments
with nucleos(t)ide analogue (NA) and/or interferon-α (IFN-α) (4-10). It is therefore
important to identify the HBV-infected patients who are more likely to develop HCC,
allowing timely intervention in those who will benefit most.
Epidemiological cohort studies have demonstrated that male gender, increasing age,
cirrhosis, high viral load (≥104 copies/ml), hepatitis B e antigen (HBeAg) expression,
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

7
HBV genotype C2 (vs. genotype B2), low albumin, and elevated alanine
aminotransferase (ALT) increase the risk of HCC in chronic HBV-infected patients
(11-15). Some of these risk factors have been utilized to construct clinical scoring
systems for the prediction of HCC (12-15). However, HBeAg sero-status and the
levels of HBV DNA and ALT are usually changeable during the long-term HBV
infection, and differ among the patients infected with different HBV genotypes, which
might result in low discriminatory performance in different populations (16-21).
Therefore, more robust biomarkers are needed to improve the prediction power of the
current clinical scoring systems.
HBV demonstrates “mutation-selection-adaptation”, a viral evolutionary process
involved in hepatocarcinogenesis. During this process, HBV accumulates HCC-risk
mutations, predominantly in the core promoter region of HBV genome (22-26). Of
these mutations, A1762T/G1764A has been prospectively shown to be an independent
risk factor of HCC (15,26). A1762T/G1764A and A1762T/G1764A-based combo
mutants are potentially selected by the immunocompromised microenvironment
predisposed by genetic polymorphisms of key immune and proinflammatory
molecules, and in turn promote an aggressive phenotype of HCC, as well as the
recurrence of HCC after curative surgery (27-30). The objective of this study was to
clarify if the baseline HBV mutations can predict the outcome of HBV-infected
patients and if HCC risk contributed by the HBV mutations can be selectively reduced
by antiviral treatment. This study should lay foundation for effective prediction and
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

8
specific prophylaxis of HCC in HBV-infected patients.
Materials and Methods
Cohort enrollment
This mixed cohort study was initiated in January 2008 and approved by the
institutional review board of Second Military Medical University. From August 1998
to December 2007, 3304 consecutive chronic HBV-infected patients admitted to the
Department of Infectious Diseases, the 2nd Affiliated Hospital of this university were
invited to participate in this study. Patients were included in the study if (i) they were
newly diagnosed as chronic hepatitis B; (ii) they provided sufficient cryopreserved
sera from peripheral blood harvested within 2 weeks before antiviral treatment or
during their initial visit; and (iii) they provided written informed consents. Patients
were excluded from the study if (i) they had decompensated liver cirrhosis or HCC; (ii)
they were co-infected with hepatitis A virus, hepatitis C virus, hepatitis D virus,
hepatitis E virus, human immunodeficiency virus, and/or Treponema pallidum; (iii)
they had autoimmune liver diseases; and (iv) they received antiviral treatment before
enrollment. Chronic hepatitis B, liver cirrhosis, and HCC were diagnosed as
previously described (25). Cirrhotic patients manifested with ascites, jaundice,
variceal bleeding or hepatic encephalopathy were diagnosed as decompensated
cirrhosis. A total of 2512 eligible patients were initially enrolled.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

9
Collection of baseline demographic and clinical data
A structured questionnaire was designed to extract baseline data of study participants
from their medical records. Data collected include sociodemographics, smoking,
alcohol consumption, medical history, and biochemical parameters from blood tests
such as liver function, antibodies, and platelet count within 2 weeks before antiviral
treatment or at their first admission. Microbiological and biochemical parameters
were tested as previously described (25).
HBV genotyping and mutation assay
HBV DNA was extracted from frozen sera, quantified twice using quantitative PCR,
and genotyped as previously described (20). The core promoter region from nt.1626 to
nt.2004 of HBV genome was amplified using nested PCR and directly sequenced or
sequenced after cloning (25,31). The sequences were aligned and analyzed using
MEGA5.0 and Bioedit 7.0 software packages and deposited in GenBank with
accession numbers KF164837-KF166793. A total of 18 “hotspots” with a mutation
frequency of >10% in this region as previously detailed (25) were evaluated.
Antiviral treatment
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

10
Antiviral treatment was administered according to disease indications as well as
patients’ willingness, compliance, and cost. Generally, patients were suggested to
receive antiviral treatment if they had high serum ALT (≥twice the upper limit of
normal) and elevated HBV DNA titer (≥105 copies/mL for HBeAg-positive or ≥104
copies/mL for HBeAg-negative patients), or cirrhosis with detectable HBV DNA (32).
For oral NA treatment, lamivudine (LAM, 100mg), adefovir dipivoxil (ADV, 10mg),
entecavir (ETV, 0.5mg), or telbivudine (LdT, 600mg) was given daily for ≥48 weeks.
Adding-on or switch-to ADV was adopted as a rescue therapy for patients with viral
breakthrough and/or drug-resistant mutations under LAM, LdT or ETV treatment, and
vice versa. For cirrhosis-free patients who were resistant to LAM, recombinant
IFN-α1b was given if their liver function permitted. Intramuscular injection of
recombinant IFN-α1b (5MU every other day) and subcutaneous administration of
pegylated IFN-α (Peg-IFN-α2a, 180µg/week; Peg-IFN-α2b, 1.5µg/kg body
weight/week) were adopted. A 48-week IFN-treatment course was essential for most
patients. For those who had partial virological responses at week 24 of treatment,
IFN-α course was prolonged to 72 weeks. Patients who did not respond to antiviral
treatment mostly failed to complete antiviral treatment for ≥48 weeks and were
excluded from the final analysis.
Follow-up
Participants received regular follow-up examinations at our outpatient clinics or at
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

11
their local tertiary hospitals. We collected information including real-life regimens of
antiviral treatment, liver function test results, and medical imaging findings by
checking their medical records. Information regarding HCC occurrence and death
before January 2008 was obtained through Shanghai Cancer Registry and Death
Certification System. Information regarding HCC occurrence and death after January
2008 was obtained by conducting regular telephone interviews, and/or household
visits. The follow-up was finished on May 31, 2013. Causes of death were determined
according to the primary diagnosis of hospitalization within 3 months before death.
The primary outcome was HCC occurrence. Death from HCC, decompensated
cirrhosis, and/or liver failure was termed as liver death. All participants were
self-reported Han Chinese.
Statistical analysis
Categorical variables were compared using chi-square test. Patients who survived or
died of other causes were censored at their last follow-up visit. Kaplan-Meier method
was applied to estimate the cumulative incidences of HCC and liver death, and
log-rank test was performed to compare the survival curves. The hazard ratio (HR)
and 95% confidence interval (CI) were calculated using the Cox proportional hazard
model. The significant factors in the univariate Cox analysis were introduced into the
multivariate Cox model to determine the factors independently contributing to HCC
occurrence and liver death. To evaluate the prophylactic effect of antiviral treatments
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

12
on HCC and liver death, the propensity score (PS) matching method was used to
balance baseline variables between antiviral and control cohorts. A PS was estimated
for all patients with antiviral treatments using multiple logistic regression analysis.
Variables used in the model were age, gender, cirrhosis, HBV genotype, HBeAg,
HBV DNA, ALT, aspartate aminotransferase (AST), total bilirubin, direct bilirubin,
albumin, and platelet count. We performed the nearest available matching on the PS,
as described by Hosaka, et al (6). Demographic (gender, age, and cirrhosis) and all
factors (gender, age, cirrhosis, C1653T, T1753V, and A1762T/G1764A) that
independently increased HCC risk were introduced into the multivariate Cox model to
re-calculate regression coefficient (β) of each variable, respectively. Projected HCC
risk based on demographic and all independent risk factors were calculated using the
equations: demographic=∑βi×Xi (Xi: gender, age, and cirrhosis), and all independent
risk factors=∑βj×Xj (Xj: gender, age, cirrhosis, C1653T, T1753V, and
A1762T/G1764A). Discrimination was analyzed using receiver operating
characteristic (ROC). Area under ROC curve (AUC) was applied to evaluate if the
HBV mutations could improve the prediction power of the demographic factors. All
analyses were two-sided and conducted using SPSS version 18.0 for Windows (SPSS,
Chicago, IL), R (http://www.r-project.org/), and medcalc (http://www.medcalc.org/).
Significance was set as P<0.05.
Results
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

13
Patient characteristics
Of 2512 eligible patients, 398 were excluded (Supplementary Figure 1). There were
no statistical differences in age, gender, cirrhosis, and major liver function parameters
between the enrolled and excluded patients (data not shown). The remaining 2114
patients were followed-up for a mean of 8.92 years (IQR, 6.67-11.00 years). Table 1
shows baseline characteristics and follow-up data of the study patients. Of the 2114
patients, 209 developed HCC during 18406 person-years of follow-up (incidence:
11.36/1000 person-years); 361 died of HBV-related liver diseases (mortality:
19.61/1000 person-years). Of 612 patients with antiviral treatment, 153 were treated
with IFN-α alone, 380 treated with NAs alone, and 79 treated with IFN-α plus NAs.
Antiviral treatment significantly reduced HCC occurrence and liver death. HBV
mono-genotype was identified in 1659 (78.48%) patients. HBV genotype B2
accounted for 26.94%; and genotype C2, 73.06%.
The PS matching with key baseline characteristics was applied to allow a common
background for comparison between antiviral and control cohorts, resulting in a
matched sample size with 521 patients in each cohort. In the antiviral cohort, 109
were treated with IFN-α alone, 347 treated with NAs alone, and 65 treated with IFN-α
plus NAs. Antiviral treatment significantly reduced HCC incidence and liver death in
the matched cohorts.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

14
Factors affecting HCC occurrence and liver death
Univariate Cox analyses including the baseline characteristics of 2114 patients
showed that male gender, increasing age, cirrhosis, HBV genotype C2, high direct
bilirubin (>7 μmol/L), low albumin (<35 g/L), high AFP (>20 ng/mL), low platelet
count (<100×109/L), and HBV mutations (C1653T, T1674CG, T1753V, and
A1762T/G1764A) were significant risk factors for HCC development; whereas
antiviral treatment was a protective factor of HCC. HBeAg and viral load were not
statistically associated with HCC, even in 1502 control patients without antiviral
treatment (data not shown). Multivariate Cox analysis indicated that male, age (≥40
yrs), cirrhosis, C1653T, T1753V, and A1762T/G1764A independently increased the
risk of HCC (Table 2).
Univariate Cox analysis using the baseline characteristics of 2114 patients indicated
that male, age (≥40 yrs), HBV DNA (≥106 copies/mL), AST (>37 U/L), total bilirubin
(>20 μmol/L), direct bilirubin (>7 μmol/L), albumin (<35 g/L), AFP (>20 ng/mL),
platelet count (<100×109/L), and the presence of cirrhosis, C1653T, T1674CG,
T1753V, and A1762T/G1764A were significant risk factors, whereas antiviral
treatment was a protective factor for liver death. Multivariate Cox analysis showed
that male, age (≥40 yrs), albumin (<35g/L), and platelet count (<100×109/L) were
independently risk factors, whereas antiviral treatment was an independent protective
factor for liver death (Supplementary Table 1).
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

15
Baseline combo HBV mutations cumulatively increased the occurrences of HCC
and liver death and significantly improved HCC prediction by demographic
factors in control cohort
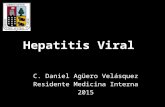
Patients with A1762T/G1764A had significantly higher cumulative risks of HCC and
liver death compared to patients without A1762T/G1764A. Furthermore, in patients
with A1762T/G1764A, addition of C1653T and/or T1753V significantly increased the
risks of HCC (HR=1.57, 95% CI=1.03-2.41; P=0.038) and liver death (HR=1.56,
95% CI=1.02-2.40; P=0.040). In genotype C2 HBV-infected patients with
A1762T/G1764A, addition of C1653T and/or T1753V significantly increased HCC
risk (HR=1.77, 95% CI=1.09-2.87; P=0.021). However, this effect was not found in
genotype B2 HBV-infected patients, possibly because of small sample size of patients
with the two or more viral mutations (Figure 1).
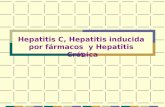
We plotted ROC curves for the development of HCC in 919 antiviral-naïve patients
(HCC, n=102) with baseline HBV mutation data. Combo HBV mutations (C1653T,
T1753V, and A1762T/G1764A) significantly improved the validity of HCC prediction
by age, gender, and cirrhosis (AUC: 0.727 vs. 0.676, P=0.002). Further stratification
analyses indicated that the combo HBV mutations significant improved the validity of
HCC prediction in genotype C2 HBV-infected patients (HCC incidence: 83/677), not
in genotype B2 HBV-infected patients (HCC incidence: 18/232) (Figure 2).
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

16
Prophylactic effects of antiviral treatment in those with or without baseline
cirrhosis in the PS matched cohorts
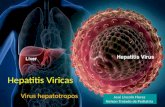
We first evaluated the prophylactic effects of antiviral treatment in 236 patients with
cirrhosis. Compared to the matched controls, antiviral treatment did not affect HCC
occurrence but significantly reduced death (HR=0.49, 95% CI=0.29-0.81; P=0.005).
The survival benefit was observed in those treated with NAs alone (n=98), but not in
those treated with IFN-α (n=12) or with IFN-α plus NAs (n=8). NA treatment for
12-59 months (n=66) did not significantly reduce HCC occurrence and liver death;
whereas NA treatment for ≥60 months (n=32) had significant prophylactic effects on
HCC occurrence and liver death. In 806 patients without cirrhosis, antiviral treatment
significantly reduced HCC occurrence (HR=0.47, 96% CI=0.26-0.85; P=0.012) and
liver death (HR=0.50, 95% CI=0.32-0.77; P=0.002); interestingly, these benefits were
observed in patients treated with IFN-α alone (n=97) or IFN-α plus NAs (n=57), but
not in those treated with NAs alone (n=249); NA treatment for ≥60 months (n=77) did
not affect HCC occurrence but significantly reduced liver death (Figure 3).
Impact of the HBV mutations on HCC occurrence and liver death were
selectively repressed by antiviral treatment in the PS matched cohorts
We compared the effects of antiviral treatment on HCC occurrence and liver death of
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

17
patients with one or more mutations (C1653T, T1753V, and A1762T/G1764A) and
patients without any of them. Antiviral treatment significantly reduced HCC
occurrence in those with the HBV mutation(s), but did not reduce HCC risk in those
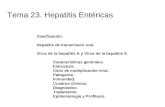
without (Supplementary Figure 2). In patients with A1762T/G1764A, antiviral
treatment significantly reduced HCC occurrence, whereas in patients without
A1762T/G1764A, antiviral treatment did not reduce HCC occurrence; similar results
were obtained in patients with or without C1653T; interestingly, in patients with
T1753V, antiviral treatment did not reduce HCC occurrence, whereas in those without
T1753V, antiviral treatment significantly reduced HCC occurrence (Figure 4).
Antiviral treatment significantly reduced liver death in patients with and without
A1762T/G1764A or C1653T mutations. However, antiviral treatment did not affect
liver death in patients with T1753V, but reduced liver death in those without T1753V
(Supplementary Figure 3).
Factors affecting the prophylactic effect of antiviral treatments
We then assessed baseline factors affecting the prophylactic effect of antiviral
treatments in 612 patients with antiviral treatment. Multivariate Cox analyses showed
that age (≥60 yrs), male, and the presence of cirrhosis and T1753V independently
predicted HCC development (Supplementary Table 2); while age (≥60 yrs), male, and
T1753V independently predicted liver death (Supplementary Table 3).
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

18
Discussion
In this study, male, age, cirrhosis, C1653T, T1753V, and A1762T/G1764A were found
to be independent risk factors of HCC in HBV-infected patients. High viral load, a
well-established risk factor of HCC (11-14), did not significantly increase HCC risk in
this study. The same was true for HBeAg, another risk factor of HCC (33). These
inconsistencies were also reported in the constituents of the HCC scoring systems
developed from hospital-based and community-based studies in East Asia (12-15),
possibly because these covariates were collected at different time points during
chronic HBV infection. In the natural history of chronic HBV infection, viral load can
be high (106-1010 copies/mL) at HBeAg-positive stage, and then decreases
dramatically (104-108 copies/mL) or fluctuates after HBeAg seroconversion (16). To
determine the contribution of HBV replication to HCC risk in HBV-infected subjects,
it may be better to determine the baseline HBV DNA level after HBeAg
seroconversion. Furthermore, age, male, HBeAg, HBV genotype C, abnormal ALT,
and high viral load can also predict the development of cirrhosis (14), a benign
disease vastly different from HCC, indicating that the current scoring systems based
on these demographic and clinical variables is not specific for HCC. During chronic
HBV infection, the HCC-risk HBV mutations including A1762T/G1764A, C1653T,
and T1753V accumulate consecutively prior to HCC occurrence. A1762T/G1764A is
an earlier generated HCC-risk mutation, whereas C1653T and T1753V are later
generated ones (25,31,34). Furthermore, HBV combo mutations have higher
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

19
specificities than single ones in indicating HCC (24,25). These HBV mutations
accumulated during this evolutionary process should be more robust and more
specific than those changeable clinical markers in predicting HCC occurrence. The
HBV combo mutations significantly improved HCC prediction using the 3 significant
demographic factors (Figure 2). Thus, the HBV combo mutations should be
incorporated into the current risk prediction models to improve the prediction of HCC
in HBV-infected patients.
HBV X protein (HBx) contributes centrally to HCC development at least partially via
up-regulating HBx-induced cyclin D1 (35). HBV 1753/1762/1764 mutations at the
C-terminal of HBx are associated with active viral replication in human hepatoma cell
lines (36). It had been shown that A1762T/G1764A-based HBV combo mutants,
rather than those with A1762T/G1764A alone, accelerate p21 degradation and
stimulate expression of S-phase kinase-associated protein 2 in hepatocytes or HCC
cells (29). These data may help in explaining why A1762T/G1764A-based combo
mutation was more effective than A1762T/G1764A alone in predicting HCC and liver
death.
Following the identification of high-risk HBV-infected patients, it becomes
indispensible to develop an effective prophylactic option on HCC or liver death in
patients with these viral mutations. We found, for the first time, that antiviral
treatment significantly reduced HCC development in HBV-infected patients carrying
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

20
A1762T/G1764A or C1653T mutation. These data indicate that HBV with
A1762T/G1764A and/or C1653T mutations has a more potent carcinogenic potential
than its wild-type counterparts and also responds efficiently to standard antiviral
treatment. Interestingly, the risk of HCC contributed by HBV T1753V mutation can
not be significantly reduced by standard antiviral treatment. The reason remains
unknown. We hypothesize that T1753V mutation introduces a novel drug-resistant
capacity of HBV or some idiopathetic drug-resistant mutations in HBV genome are
synchronously generated with T1753V during this revolutionary process. Further
studies are needed to address this issue. Therefore, HBV-infected patients with
A1762T/G1764A or C1653T should be given priority of receiving antiviral treatment;
while patients with T1753V should be monitored frequently to identify early,
resectable HCC.
Our stratification analysis indicated that the combo mutations significantly improved
HCC prediction in genotype C2 HBV-infected patients, but not in genotype B2
HBV-infected patients. A1762T/G1764A significantly increased HCC risk and liver
death in genotype B2 HBV-infected patients (Figure 1C, 1D). Genotype B2 HBV has
a relative weaker carcinogenic potential than does genotype C2, possibly because
genotype B2 has less HCC-related mutations. A1762T/G1764A is more frequent in
HBV genotypes C and D than in genotypes A and B (37). Although the HBV
mutations increase with increasing age of HCC-free HBV-infected subjects, the HBV
mutations such as A1762T/G1764A and T1753V are extremely higher in younger
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

21
HBV-HCC patients, compared to the age-matched HCC-free HBV-infected subjects
(25). The HBV mutations independently predicted HCC occurrence (Table 2). Thus,
the HBV mutations, whose patterns differ among HBV genotypes, are HCC-specific
and the association of A1762T/G1764A-based HBV mutations with HCC risk may be
generalized to populations with different HBV genotypes.
The minimum period for NA treatment required to reduce HCC occurrence in
HBV-infected patients differs greatly among studies carried out in Taiwan (≥90 days),
USA (45 months), Japan (≥48 weeks), and South Korea (≥24 weeks) (4-7). Our data
indicated that NA treatment for ≥60 months was required for the prophylaxis of HCC
in cirrhotic patients. IFN-α treatment independently suppressed the development of
HCC in non-cirrhotic HBV-infected patients. This is supported by the fact that HBV
genotype B2 is less apt to cause cirrhosis and more sensitive to IFN-α treatment than
genotype C2 (38,39). Thus, these data are particularly important for the prophylaxis of
HCC in chronic HBV-infected patients.
This study has several limitations. First, 701 patients meeting the current standard for
antiviral treatment had not received antiviral treatment. Second, data concerning
fibrosis stage, maternal HBsAg status, family history of HCC, and quantitative
HBsAg were incomplete and therefore not included in the analyses.
In conclusion, baseline combo mutations in the core promoter region of HBV genome
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

22
are more effective than A1762T/G1764A alone in predicting HCC occurrence and
liver death and significantly improve HCC prediction by well-established
demographic factors. Antiviral treatment was extremely effective in reducing HCC
occurrence in chronic HBV-infected patients carrying A1762T/G1764A or C1653T
but not in those carrying T1753V mutation. These data are helpful for effective
prediction and specific prophylaxis of HCC and liver death.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

23
Acknowledgements
We gratefully acknowledge Drs. Hua Wang, Weiwei Gong, and experts responsible
for the maintenance of Cancer Registry and Death Certification Systems of Shanghai
for their great help in the follow-up study. We regret that some articles relevant to this
study are not cited due to space limitations.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

24
References
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics.
CA Cancer J Clin 2011;61:69-90.
2. Huang YT, Jen CL, Yang HI, Lee MH, Su J, Lu SN, et al. Lifetime risk and sex
difference of hepatocellular carcinoma among patients with chronic hepatitis B
and C. J Clin Oncol 2011;29:3643-50.
3. Han X, Huang CX, Zhang HW, Qiao P, Xie M, Zhang R, et al. The occurrence and
survival condition of primary liver cancer among residents in Yangpu district of
Shanghai between 2002 and 2010. Chin J Prev Med 2012;46:119-124 [in Chinese]
4. Wu CY, Lin JT, Ho HJ, Su CW, Lee TY, Wang SY, et al. Association of
nucleos(t)ide analogue therapy with reduced risk of hepatocellular carcinoma in
patients with chronic hepatitis B: a nationwide cohort study. Gastroenterology
2014;147:143-51.e5.
5. Gordon SC, Lamerato LE, Rupp LB, Li J, Holmberg SD, Moorman AC, et al.
Antiviral therapy for chronic hepatitis B virus infection and development of
hepatocellular carcinoma in a US population. Clin Gastroenterol Hepatol
2014;12:885-93.
6. Hosaka T, Suzuki F, Kobayashi M, Seko Y, Kawamura Y, Sezaki H, et al.
Long-term entecavir treatment reduces hepatocellular carcinoma incidence in
patients with hepatitis B virus infection. Hepatology 2013;58:98-107.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

25
7. Cho JY, Paik YH, Sohn W, Cho HC, Gwak GY, Choi MS, et al. Patients with
chronic hepatitis B treated with oral antiviral therapy retain a higher risk for HCC
compared with patients with inactive stage disease. Gut 2014;63:1943-50.
8. van Zonneveld M, Honkoop P, Hansen BE, Niesters HG, Darwish Murad S, de Man
RA, et al. Long-term follow-up of alpha-interferon treatment of patients with
chronic hepatitis B. Hepatology 2004;39:804-10.
9. Yin J, Li N, Han Y, Xue J, Deng Y, Shi J, et al. Effect of antiviral treatment with
nucleotide/nucleoside analogs on postoperative prognosis of hepatitis B
virus-related hepatocellular carcinoma: a two-stage longitudinal clinical study. J
Clin Oncol 2013;31:3647-55.
10. Qu LS, Jin F, Huang XW, Shen XZ. Interferon-α therapy after curative resection
prevents early recurrence and improves survival in patients with hepatitis B
virus-related hepatocellular carcinoma. J Surg Oncol 2010;102:796-801.
11. Chan HL, Tse CH, Mo F, Koh J, Wong VW, Wong GL, et al. High viral load and
hepatitis B virus subgenotype ce are associated with increased risk of
hepatocellular carcinoma. J Clin Oncol 2008;26:177-82.
12. Wong VW, Chan SL, Mo F, Chan TC, Loong HH, Wong GL, et al. Clinical
scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers.
J Clin Oncol 2010;28:1660-5.
13. Yang HI, Yuen MF, Chan HL, Han KH, Chen PJ, Kim DY, et al. Risk estimation
for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

26
validation of a predictive score. Lancet Oncol 2011;12:568-574.
14. Lee MH, Yang HI, Liu J, Batrla-Utermann R, Jen CL, Iloeje UH, et al. Prediction
models of long-term cirrhosis and hepatocellular carcinoma risk in chronic
hepatitis B patients: risk scores integrating host and virus profiles. Hepatology
2013;58:546-54.
15. Yuen MF, Tanaka Y, Fong DY, Fung J, Wong DK, Yuen JC, et al. Independent risk
factors and predictive score for the development of hepatocellular carcinoma in
chronic hepatitis B. J Hepatol 2009;50:80-88.
16. Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special
emphasis on disease progression and prognostic factors. J Hepatol
2008;48:335-52.
17. Spradling PR, Bulkow L, Teshale EH, Negus S, Homan C, Simons B, et al.
Prevalence and causes of elevated serum aminotransferase levels in a
population-based cohort of persons with chronic hepatitis B virus infection. J
Hepatol 2014;61:785-91.
18. Tohme RA, Bulkow L, Homan CE, Negus S, McMahon BJ. Rates and risk factors
for hepatitis B reactivation in a cohort of persons in the inactive phase of chronic
hepatitis B-Alaska, 2001-2010. J Clin Virol 2013;58:396-400.
19. Croagh CM, Bell SJ, Chen RY, Locarnini S, Desmond PV. Longitudinal
observation of viral load changes in untreated HBeAg negative chronic hepatitis B.
Acta Gastroenterol Belg 2013;76:275-81.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

27
20. Yin J, Zhang H, He Y, Xie J, Liu S, Chang W, et al. Distribution and
hepatocellular carcinoma-related viral properties of hepatitis B virus genotypes in
Mainland China: a community-based study. Cancer Epidemiol Biomarkers Prev
2010;19:777-86.
21. Arends P, Sonneveld MJ, Zoutendijk R, Carey I, Brown A, Fasano M, et al.
Entecavir treatment does not eliminate the risk of hepatocellular carcinoma in
chronic hepatitis B: limited role for risk scores in Caucasians. Gut
2015;64:1289-95.
22. Takahashi K, Akahane Y, Hino K, Ohta Y, Mishiro S. Hepatitis B virus genomic
sequence in the circulation of hepatocellular carcinoma patients: comparative
analysis of 40 full-length isolates. Arch Virol 1998;143:2313-26.
23. Baptista M, Kramvis A, Kew MC. High prevalence of 1762(T) 1764(A) mutations
in the basic core promoter of hepatitis B virus isolated from black Africans with
hepatocellular carcinoma compared with asymptomatic carriers. Hepatology
1999;29:946-53.
24. Liu S, Zhang H, Gu C, Yin J, He Y, Xie J, et al. Associations between hepatitis B
virus mutations and the risk of hepatocellular carcinoma: a meta-analysis. J Natl
Cancer Inst 2009;101:1066-82.
25. Yin J, Xie J, Liu S, Zhang H, Han L, Lu W, et al. Association between the various
mutations in viral core promoter region to different stages of hepatitis B, ranging
of asymptomatic carrier state to hepatocellular carcinoma. Am J Gastroenterol
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

28
2011;106:81-92.
26. Fang ZL, Sabin CA, Dong BQ, Ge LY, Wei SC, Chen QY, et al. HBV A1762T,
G1764A mutations are a valuable biomarker for identifying a subset of male
HBsAg carriers at extremely high risk of hepatocellular carcinoma: a prospective
study. Am J Gastroenterol 2008;103:2254-62.
27. Zhang Q, Yin J, Zhang Y, Deng Y, Ji X, Du Y, et al. HLA-DP polymorphisms
affect the outcomes of chronic hepatitis B virus infections, possibly through
interacting with viral mutations. J Virol 2013;87:12176-86.
28. Zhang Q, Ji XW, Hou XM, Lu FM, Du Y, Yin JH, et al. Effect of functional
nuclear factor-kappaB genetic polymorphisms on hepatitis B virus persistence and
their interactions with viral mutations on the risk of hepatocellular carcinoma. Ann
Oncol 2014;25:2413-9.
29. Huang Y, Tai AW, Tong S, Lok AS. HBV core promoter mutations promote
cellular proliferation through E2F1-mediated upregulation of S-phase
kinase-associated protein 2 transcription. J Hepatol 2013;58:1068-73.
30. Yeh CT, So M, Ng J, Yang HW, Chang ML, Lai MW, et al. Hepatitis B virus-DNA
level and basal core promoter A1762T/G1764A mutation in liver tissue
independently predict postoperative survival in hepatocellular carcinoma.
Hepatology 2010;52:1922-33.
31. Li Z, Xie Z, Ni H, Zhang Q, Lu W, Yin J, et al. Mother-to-child transmission of
hepatitis B virus: Evolution of hepatocellular carcinoma-related viral mutations in
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

29
the post-immunization era. J Clin Virol 2014;61:47-54.
32. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology
2009;50:661-2.
33. Yang HI, Lu SN, Liaw YF, You SL, Sun CA, Wang LY, et al. Hepatitis B e antigen
and the risk of hepatocellular carcinoma. N Engl J Med 2002;347:168-74.
34. Bai X, Zhu Y, Jin Y, Guo X, Qian G, Chen T, et al. Temporal acquisition of
sequential mutations in the enhancer II and basal core promoter of HBV in
individuals at high risk for hepatocellular carcinoma. Carcinogenesis
2011;32:63-8.
35. Chen X, Zhang L, Zheng S, Zhang T, Li M, Zhang X, et al. Hepatitis B Virus X
Protein Stabilizes Cyclin D1 and Increases Cyclin D1 Nuclear Accumulation
through ERK-Mediated Inactivation of GSK-3β. Cancer Prev Res (Phila)
2015;8:455-63.
36. Parekh S, Zoulim F, Ahn SH, Tsai A, Li J, Kawai S, et al. Genome replication,
virion secretion, and e antigen expression of naturally occurring hepatitis B virus
core promoter mutants. J Virol 2003;77:6601-12.
37. Liu CJ, Kao JH. Global perspective on the natural history of chronic hepatitis B:
role of hepatitis B virus genotypes A to J. Semin Liver Dis 2013;33:97-102.
38. Chan HL, Wong GL, Tse CH, Chim AM, Yiu KK, Chan HY, et al. Hepatitis B
virus genotype C is associated with more severe liver fibrosis than genotype B.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

30
Clin Gastroenterol Hepatol 2009;7:1361-6.
39. Wai CT, Chu CJ, Hussain M, Lok AS. HBV genotype B is associated with better
response to interferon therapy in HBeAg(+) chronic hepatitis than genotype C.
Hepatology 2002;36:1425-30.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

31
FIGURE LEGENDS
Figure 1. Impact of baseline C1653T, T1753V, and A1762T/G1764A mutations on
HCC occurrence and liver death in control patients. (A) HCC occurrence in patients
with mutation data; (B) liver death in patients with mutation data; (C) HCC
occurrence in genotype B2 HBV-infected patients; (D) liver death in genotype B2
HBV-infected patients. (E) HCC occurrence in genotype C2 HBV-infected patients; (F)
liver death in genotype C2 HBV-infected patients. P values, log-rank test.
Figure 2. Comparison of HCC prediction by baseline demographic factors (age,
gender, and cirrhosis) with and without baseline combo mutations of HBV in control
patients. (A) All patients with mutation data; (B) Genotype B2 HBV-infected patients;
(C) Genotype C2 HBV-infected patients.
Figure 3. The effects of antiviral treatment on HCC occurrence and liver death in
patients with or without liver cirrhosis in the PS matched cohorts. (A) NA treatment
on HCC occurrence in cirrhotic patients; (B) NA treatment on liver death in cirrhotic
patients; (C) Antiviral treatment on HCC occurrence in non-cirrhotic patients; (D)
Antiviral treatment on liver death in non-cirrhotic patients; (E) NA treatment on HCC
occurrence in non-cirrhotic patients; and (F) NA treatment on liver death in
non-cirrhotic patients. P values, log-rank test.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

32
Figure 4. Effect of antiviral treatment on HCC occurrence in chronic HBV-infected
patients with and without each of the HCC-risk mutations in the PS matched cohorts.
(A) patients with A1762T/G1764A; (B) patients without A1762T/G1764A; (C)
patients with C1653T; (D) patients without C1653T; (E) patients with T1753V; (F)
patients without T1753V. P values, log-rank test.
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

Table 1. Baseline characteristics and follow-up summary of study patients a
Variables
Entire Cohort Propensity Score Match Cohort
Control cohort
(n=1502)
Antiviral-treated
cohort (n=612) P
Control cohort
(n=521)
Antiviral-treated
cohort (n=521) P
Age (years)
<40 567(37.7) 345(56.4) <0.001 258(49.5) 275(52.8) 0.55
40-59 741(49.3) 232(37.9) 224(43.0) 212(40.7)
≥60 194(12.9) 35(5.7) 39(7.5) 34 (6.5)
Gender (Male) 1119(74.5) 505(82.5) <0.001 432(82.9) 430(82.5) 0.87
HBV genotype
B 289(19.2) 158(25.8) 0.15 126(24.2) 140(26.9) 0.58
C 829(55.2) 383(62.6) 324(62.2) 316(60.7)
Unclassified 384(25.6) 71(11.6) 71(13.6) 65(12.5)
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

HBeAg positivity 490(32.6) 324(52.9) <0.001 253(48.6) 262(50.3) 0.58
Cigarette smoking 342(22.8) 129(21.1) 0.40 404(77.5) 415(79.7) 0.41
Alcohol drinking 309(20.6) 106(17.3) 0.09 105(20.2) 88(16.9) 0.18
Cirrhosis 362(24.1) 128(20.9) 0.12 118(22.6) 118(22.6) 1.000
HBV DNA (log10 copies/mL)
<6.0 905(60.3) 242(39.5) <0.001 208(39.9) 229(44.0) 0.29
≥6.0 597(39.7) 370(60.5) 313(60.1) 292(56.0)
Total bilirubin (μmol/L)
≤20 329(22.1) 180(30.0) <0.001 126(24.2) 127(24.4) 0.94
>20 1160(77.9) 420(70.0) 395(75.8) 394(75.6)
Direct bilirubin (μmol/L)
≤7 452(30.4) 239(39.8) <0.001 174(33.4) 176(33.8) 0.90
>7 1035(69.6) 361(60.2) 347(66.6) 345(66.2)
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

Albumin (g/L)
≥35 921(61.6) 414(67.8) 0.007 333(63.9) 346(66.4) 0.40
<35 575(38.4) 197(32.2) 188(36.1) 175(33.6)
Alanine aminotransferase (U/L)
≤40 381(25.7) 94(15.7) <0.001 87(16.7) 92(17.7) 0.68
>40 1103(74.3) 506(84.3) 434(83.3) 429(82.3)
Aspartate aminotransferase (U/L)
≤37 300(22.9) 80(13.7) <0.001 67(12.9) 77(14.8) 0.37
>37 1010(77.1) 504(86.3) 454(87.1) 444(85.2)
Platelet count (109/L)
100-300 698(46.5) 306(50.0) 0.14 245(47.0) 251(48.2) 0.71
<100 804(53.5) 306(50.0) 276(53.0) 270(51.8)
Person-years of follow-up 13285 5121 4387 4287
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

Follow-up duration (years)b 9.2(7.0-11.3) 8.2(6.3-10.6) 8.83(6.8-10.7) 8.17(6.3-10.4)
Hepatocellular carcinoma 173(11.5) 36(5.9) <0.001 61(11.7) 33(6.3) 0.002
Incidence (/1000 person-years) 13.02 7.02 0.001 13.90 7.70 0.005
Death from Liver Diseases 304(20.2) 57(9.3) <0.001 107(20.5) 54(10.4) <0.001
Fatality (/1000 person-years) 22.88 11.13 <0.001 24.39 12.60 <0.001
NOTE: a Data are number (%), unless otherwise indicated. Some percentages do not sum up to 100 because of rounding. b Median (IQR)
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

Table 2. Cox analysis of factors significantly affected hepatocellular carcinoma occurrence in patients with chronic HBV infection a
Variable
No.(%) of
participants
(n=2114)
Person-years
of follow-up
No.
of
HCC
Incidence per
1000
person-years
Univariate
analysis
HR (95% CI)
P
Multivariate
analysis
HR (95% CI) c
P
Gender
Female 490(23.2) 4364 24 5.50 1.00 1.00
Male 1624(76.8) 14042 185 13.17 2.91(1.90-4.47) <0.001 3.10(1.76-5.45) <0.001
Age (years)
<40 912(43.1) 8473 54 6.37 1.00 1.00
40-59 973(46.0) 8123 123 15.14 2.58(1.87-3.55) <0.001 2.09(1.35-3.23) 0.001
≥60 229(10.8) 1809 32 17.69 3.44(2.21-5.36) <0.001 2.44(1.29-4.61) 0.006
Cirrhosis
No 1624(76.8) 14698 115 7.82 1.00 1.00
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

Yes 490(23.2) 3709 94 25.34 2.94(2.22-3.89) <0.001 1.89(1.21-2.96) 0.005
HBV genotype
B 447(26.9) 3812 25 6.56 1.00
C 1212(73.1) 10752 125 11.63 1.61(1.05-2.48) 0.03
Antiviral therapy
No 1502(71.0) 13276 172 13.02 1.00 1.00
Yes 612(29.0) 5132 36 7.01 0.60(0.42-0.86) 0.006 0.64(0.41-1.00) 0.050
Direct bilirubin (μmol/L)
≤7 691(33.1) 6440 51 7.92 1.00
>7 1396(66.9) 11751 158 13.45 1.41(1.02-1.93) 0.036
Albumin (g/L)
≥35 1335(63.4) 12275 106 8.64 1.00
<35 772(36.6) 6073 102 16.80 1.68(1.27-2.22) <0.001
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

α- fetoprotein (ng/mL)
≤20 1358(64.4) 12064 115 9.53 1.00
20-400 752(35.6) 6315 94 14.89 1.49(1.13-1.95) 0.004
Platelet count (109/L)
100-300 1004(47.5) 8960 66 7.37 1.00
<100 1110(52.5) 9445 143 15.14 1.83(1.36-2.45) <0.001
C1653T b
C 1166(82.3) 10410 88 8.45 1.00 1.00
T 250(17.7) 2160 47 21.76 2.43(1.70-3.48) <0.001 1.86(1.24-2.81) 0.003
T1674C/G b
T 1051(74.3) 9426 84 8.91 1.00
C or G 364(25.7) 3138 50 15.93 1.67(1.18-2.38) 0.004
T1753V b
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

T 1180(83.9) 10530 96 9.12 1.00 1.00
V (C or A or G) 226(16.1) 1955 39 19.95 1.97(1.35-2.87) <0.001 1.58(1.03-2.43) 0.036
A1762T/G1764A b
Wild-type 549(39.8) 5086 23 4.52 1.00 1.00
Mutation 831(60.2) 7143 106 14.84 2.89(1.83-4.56) <0.001 1.96(1.18-3.26) 0.009
NOTE: a Data are number (%). b HBV mutation. c Only included significant covariates in univariate analysis.
Cancer R
esearch. on D
ecember 7, 2020. ©
2015 Am
erican Association for
cancerpreventionresearch.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on A
ugust 19, 2015; DO
I: 10.1158/1940-6207.CA
PR
-15-0160

C
0.30
0.25
0.20
0.15
0.10
0.05
0.00
1.00
0.80
0.60
0.40
0.20
0.00
Cum
ulat
ive
Inci
denc
e of
HC
C
Cum
ulat
ive
Live
r Dis
ease
-spe
cific
Sur
viva
l
C1653T / T1753V / A1762TG1764A C1653T / T1753V / A1762TG1764AA B
Follow-up time (months) Follow-up time (months)No. at risk -/-/- 348 332 323 307 236 162 73 9-/-/+ 276 250 239 216 172 114 62 9+/-/+ or -/+/+or +/+/+ 263 230 218 192 155 102 48 6
348 332 323 310 238 163 73 9276 252 242 221 181 119 65 9
263 237 224 204 170 110 49 6
Reference -/-/-
HR 3.76 (95% CI 1.99 - 7.08),P < 0.001
HR 5.92 (95% CI 3.22 - 10.88), P < 0.001-/-/--/-/++/-/+ or -/+/+or +/+/+
-/-/--/-/++/-/+ or -/+/+or +/+/+
-/-/-, Reference-/-/+, HR 2.02 (95% CI 1.38 - 2.97), P < 0.001+/-/+ or -/+/+ or +/+/+, HR 2.64 (95% CI 1.82 - 3.83), P < 0.001
0.30
0.25
0.20
0.15
0.10
0.05
0.00
D
Follow-up time (months)Follow-up time (months)
0.30
0.25
0.20
0.15
0.10
0.05
0.00
E
Follow-up time (months)
Cum
ulat
ive
Inci
denc
e of
HC
C C
umul
ativ
e In
cide
nce
of H
CC
F
No. at risk
No. at risk
Follow-up time (months)
-/-/- 136 125 122 117 86 56 27 4-/-/+ 69 63 56 50 37 18 9 2+/-/+ or -/+/+or +/+/+ 20 17 16 14 14 10 3
-/-/- 208 203 198 187 147 103 44 5-/-/+ 204 184 180 163 132 93 52 7+/-/+ or -/+/+or +/+/+ 241 211 200 177 140 91 44 6
136 125 122 118 86 56 27 469 63 57 51 39 21 9 2
20 17 16 15 14 10 3
208 203 198 189 149 104 44 5204 186 182 167 139 95 55 7
241 218 206 188 155 99 45 6
C1653T / T1753V / A1762TG1764A in genotype B C1653T / T1753V / A1762TG1764A in genotype B
C1653T / T1753V / A1762TG1764A in genotype C C1653T / T1753V / A1762TG1764A in genotype C
-/-/--/-/++/-/+ or -/+/+or +/+/+
-/-/--/-/++/-/+ or -/+/+or +/+/+
-/-/-, Reference-/-/+, HR 2.33 (95% CI 1.23 - 4.41), P = 0.009+/-/+ or -/+/+ or +/+/+, HR 2.37 (95% CI 0.94 - 5.97), P = 0.068
-/-/-, Reference-/-/+, HR 2.04 (95% CI 1.25 - 3.34), P = 0.005+/-/+ or -/+/+ or +/+/+, HR 2.89 (95% CI 1.82 - 4.58), P < 0.001
-/-/--/-/++/-/+ or -/+/+or +/+/+
-/-/--/-/++/-/+ or -/+/+or +/+/+
Reference, -/-/-
Reference -/-/-
HR 3.61 (95% CI 0.66 - 19.72),P = 0.138
HR 3.01 (95% CI 1.41 - 6.46),P = 0.005
HR 6.21 (95% CI 1.98 - 19.51), P = 0.002
HR 5.37 (95% CI 2.63 - 10.94), P < 0.001
0 24 48 72 96 120 144 168 192
1.00
0.80
0.60
0.40
0.20
0.00
Cum
ulat
ive
Live
r Dis
ease
-spe
cific
Sur
viva
l
1.00
0.80
0.60
0.40
0.20
0.00
Cum
ulat
ive
Live
r Dis
ease
-spe
cific
Sur
viva
l
0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192 0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192 0 24 48 72 96 120 144 168 192
Figure 1
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

0.00 0.20 0.40 0.60 0.80 1.00
1.00
0.80
0.60
0.40
0.20
0.00
AUC (95% CI)
Demographics+mutations 0.727 ( 0.677 - 0.777)Demographics 0.676 ( 0.623 - 0.730)
Sens
itivi
ty
1-Specificity
P = 0.002
Demographics+mutationsDemographics
B
P = 0.119
AUC (95% CI)Demographics 0.668 (0.604 - 0.729)
Demographics+mutations 0.746 (0.685 - 0.801)
Demographics+mutationsDemographics
0.00 0.20 0.40 0.60 0.80 1.001-Specificity
1.00
0.80
0.60
0.40
0.20
0.00
Sens
itivi
ty
A
C
P = 0.005
Demographics+mutationsDemographics
AUC (95% CI)Demographics 0.677 (0.641 - 0.712)
Demographics+mutations 0.725 (0.689 - 0.758)
1.00
0.80
0.60
0.40
0.20
0.00
Sens
itivi
ty
0.00 0.20 0.40 0.60 0.80 1.001-Specificity
Figure 2
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

0.30
0.25
0.20
0.15
0.10
0.05
0.00
0.15
0.10
0.05
0.00
0.15
0.10
0.05
0.00
1.00
0.80
0.60
0.40
0.20
0.00
Cum
ulat
ive
Inci
denc
e of
HC
C C
umul
ativ
e In
cide
nce
of H
CC
Cum
ulat
ive
Inci
denc
e of
HC
C
Cum
ulat
ive
Live
r Dis
ease
-spe
cific
Sur
viva
lC
umul
ativ
e Li
ver D
isea
se-s
peci
fic S
urvi
val
Cum
ulat
ive
Live
r Dis
ease
-spe
cific
Sur
viva
l
C D
A B
E F
No. at risk Control 403 375 366 345 253 131 49 7IFN group 97 95 94 91 78 58 17 4NA group 249 239 233 199 111 54 17 1
No. at risk Control 118 95 83 71 55 32 11 112-59 mo. 66 57 51 34 22 13 2 ≥60 mo. 32 32 32 24 14 8
118 99 88 76 63 36 12 166 61 55 38 26 14 2 32 32 32 25 15 8
403 377 367 351 260 137 52 897 95 94 91 80 58 17 4
249 239 237 206 114 55 17 1
No. at risk Control 403 375 366 345 253 131 49 712-59 mon. 172 162 157 131 75 43 14 ≥60 mon. 77 77 76 68 36 11 3 1
403 377 367 351 260 137 52 8172 162 160 136 77 44 14 77 77 77 70 37 11 3 1
IFN plus NA 57 57 57 48 34 14 3 1 57 57 57 48 34 14 3 1
Control 12-59 mo.≥60 mo.
Control vs. 12-59 mo. P = 1.00Control vs. ≥ 60 mo. P = 0.03
Control 12-59 mo.≥60 mo.
Control vs. 12-59 mo. P = 0.11Control vs. ≥ 60 mo. P = 0.002
12-59 mo. vs. ≥ 60 mo. P = 0.04
12-59 mo. vs. ≥ 60 mo. P = 0.03
Control vs. IFN P = 0.01Control vs. NA P = 0.30Control vs. IFN plus NA P = 0.03 Control
IFN groupNA groupIFN plus NA
Control vs. IFN P = 0.01Control vs. NA P = 0.12Control vs. IFN plus NA P = 0.003
Control 12-59 mo.≥ 60 mo.
Control vs. 12-59 mo. P = 0.60Control vs. ≥ 60 mo. P = 0.2312-59 mo. vs. ≥ 60 mo. P = 0.37
Control 12-59 mo.≥ 60 mo.
Control vs. 12-59 mo. P = 0.63Control vs. ≥ 60 mo. P = 0.0212-59 mo. vs. ≥ 60 mo. P = 0.04
Follow-up time (months) Follow-up time (months)
Follow-up time (months) Follow-up time (months)
Follow-up time (months) Follow-up time (months)
1.00
0.80
0.60
0.40
0.20
0.00
1.00
0.80
0.60
0.40
0.20
0.00
0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 1920 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192
Control IFN groupNA groupIFN plus NA
Figure 3
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

0.25
0.20
0.15
0.10
0.05
0.00
0.25
0.20
0.15
0.10
0.05
0.00
A
Cum
ulat
ive
Inci
denc
e of
HC
C
Follow-up time (months)No. at risk Control group 222 195 182 164 127 74 27 5 Antiviral 243 229 222 193 120 70 18 2treatment
Control groupAntiviral treatment group
A1762T/G1764A - positive
C1653T - positive
Cum
ulat
ive
Inci
denc
e of
HC
C
No. at risk Follow-up time (months)
Control group 60 47 43 38 27 15 5 2
C
Antiviral 63 58 56 48 36 23 7 2 treatment
T1753V - positive
Cum
ulat
ive
Inci
denc
e of
HC
C
No. at risk Follow-up time (months)
E
Control group 62 57 54 47 39 22 8 2 Antiviral 62 58 56 47 31 17 10 3treatment
HR 0.40 (95% CI 0.22 - 0.72), P = 0.002
HR 0.45 (95% CI 0.21 - 0.98),P = 0.04
HR 1.06 (95% CI 0.44 - 2.56), P = 0.89
Control groupAntiviral treatment group
Control groupAntiviral treatment group
BA1762T/G1764A - negative
Cum
ulat
ive
Inci
denc
e of
HC
C
Control groupAntiviral treatment group
HR 1.47 (95% CI 0.51 - 4.23), P = 0.479
Follow-up time (months)
156 145 142 136 93 56 17 2 136 132 131 122 84 53 12 2
C1653T - negativeD
HR 0.57 (95% CI 0.30 - 1.07),P = 0.08
Antiviral treatment groupControl group
Cum
ulat
ive
Inci
denc
e of
HC
C
Follow-up time (months)
332 307 294 275 203 120 41 5 327 314 307 276 174 103 24 3
0.25
0.20
0.15
0.10
0.05
0.00
Control groupAntiviral treatment group
Cum
ulat
ive
Inci
denc
e of
HC
C
Follow-up time (months)
324 291 278 261 187 110 37 5 326 312 306 276 178 109 21 2
T1753V - negativeF
HR 0.42 (95% CI 0.23 - 0.77), P = 0.005
0.25
0.20
0.15
0.10
0.05
0.00
0.60
0.50
0.40
0.30
0.20
0.10
0.00
0.60
0.50
0.40
0.30
0.20
0.10
0.00
0 24 48 72 96 120 144 168 192 0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192 0 24 48 72 96 120 144 168 192
0 24 48 72 96 120 144 168 192 0 24 48 72 96 120 144 168 192
Figure 4
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160

Published OnlineFirst August 19, 2015.Cancer Prev Res Jianhua Yin, Junxue Wang, Rui Pu, et al. cohort studyactive prophylaxis of hepatocellular carcinoma: a clinic-based Hepatitis B virus combo mutations improve the prediction and
Updated version
10.1158/1940-6207.CAPR-15-0160doi:
Access the most recent version of this article at:
Material
Supplementary
60.DC1
http://cancerpreventionresearch.aacrjournals.org/content/suppl/2015/08/19/1940-6207.CAPR-15-01Access the most recent supplemental material at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.60http://cancerpreventionresearch.aacrjournals.org/content/early/2015/08/19/1940-6207.CAPR-15-01To request permission to re-use all or part of this article, use this link
Cancer Research. on December 7, 2020. © 2015 American Association forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 19, 2015; DOI: 10.1158/1940-6207.CAPR-15-0160
http://cancerpreventionresearch.aacrjournals.org/content/suppl/2015/08/19/1940-6207.CAPR-15-0160.DC1