Helicobacter pylon, Pepsinogen, and Risk for Gastric ... · sion from normal stomach to malignancy...
7
Vol. 2, 46 1 -466, September/October 1993 Cancer Epidemiology, Biomarkers & Prevention 461 I The abbreviations used are: HP, Helicobacterpylori; PG I, pepsinogen I; PG II, pepsinogen II; OR, odds ratio; CI, confidence interval. Helicobacter pylon, Pepsinogen, and Risk for Gastric Adenocarc i noma Julie Parsonnet,1 I. Michael Samloff, Lorene M. Nelson, Norman Orentreich, Joseph H. Vogelman, and Gary D. Friedman2 Division of Infectious Diseases and Geographic Medicine, Department of Medicine II. P.1 and Division of Epidemiology, Department of Health Research and Policy Ii. P., L. M. NI, Stanford University, Stanford, California 94305; Division of Gastroenterology, Sepulveda Veterans Administration Medical Center, Los Angeles, California II. M. 5.1; Orentreich Foundation for the Advancement of Science, Inc., Cold Spring-on-Hudson, New York IN. 0., 1. H. V.1; and Division of Research, Kaiser Permanente Medical Care Program, Oakland, California IC. D. F.l Abstract The objective of this project was to determine the association of Helicobacter pylon infection and serum pepsinogen levels on subsequent risk for gastric adenocarcinoma. This nested case-control study was set in a large health maintenance organization. One hundred thirty-six cases of gastric adenocarcinoma and 1 36 matched controls without adenocarcinoma from a large cohort that had contributed serum in the 1960’s were studied. The presence of lgG against H. pylon had previously been determined by enzyme-linked immunosorbent assay. Serum levels of pepsinogens I and II were ascertained by radioimmunoassay. In a sample of subjects, the presence of antiparietal cell antibodies was determined by immunofluorescent antibody assay (Nichols Laboratory). There were 98 cases of adenocarcinoma of the antrum, body, or fundus (distal cancers) and 30 of the cardia or gastroesophageal junction (proximal cancers). By univariate analysis, H. pylon infection [odds ratio (OR), 3.6; P < 0.001] and serum pepsinogen I < 50 ng/ml (OR = 2.9; P = 0.003) were both associated with development of distal cancer. In multivariate analysis, there was interaction between the two variables; H. pylon in the absence of low pepsinogen I was independently associated with cancer (OR, 2.4; P = 0.04) but low pepsinogen I in the absence of H. pylon infection was not associated with cancer (OR, 0.8; P > 0.5). In combination, however, H. pylon infection and a low pepsinogen I were associated with a marked increase in the risk of developing distal malignancy (OR, 1 0.0; P = 0.08). Low serum pepsinogen I with H. pylon infection but not in its absence is associated with a increased risk for distal gastric cancer. Received 1/25/93; revised 4/5/93; accepted 4/5/93. I To whom requestsfor reprints should be addressed, at HRP Building 2, Room 49, Stanford University, Stanford, CA 94305-5092. 1. P. is supported by an Ortho Pharmaceuticals Young Investigator Award. 2 G. D. F. is supported in part by Grant R35 CA49761 froni the National Cancer Institute. This suggests that infection rather than gastric atrophy is the determining factor in cancer risk. Introduction Of cancer precursors, among the best described histopatho- logically are those preceding adenocarcinoma of the stom- ach. In prospective and cross-sectional studies, investigators in Europe and Latin America have documented the progres- sion from normal stomach to malignancy (1 , 2). The first of the precursor lesions, chronic superficial gastritis, appears many years before cancer is manifest. It is followed by atro- phic gastnitis, intestinal metaplasia, and dysplasia. While not all precursor stages are observed in any given individual, each successive step in the sequence increases the risk of developing this malignancy (1 , 3). HP,t a bacterium that infects the mucosal lining of the stomach, causes the first of the precursor lesions, chronic superficial gastritis. Recently, three nested case-control stud- ies described an association between infection and subse- quent development of gastric cancer (4-6). Despite the dif- ferent populations evaluated (Japanese-American men in Hawaii, men in Great Britain, and men and women in Cali- fomnia), the investigators reported remarkably similar results; infection with H. py!ori was associated with a 3-6-fold in- crease in the risk of developing gastric cancer. Serum levels of pepsinogens, the proenzymes for the digestive enzyme pepsin, have also been associated with increased gastric cancer risk (7-9). Two immunochemically distinct classes of pepsinogens have been identified: PG I, which is produced in fundic mucous neck cells and in chief cells of the gastric glands, and PG II, which is produced in similar cells and in pylonic gland cells in the antrum (1 0). In atrophic gastnitis, the gastric glands have been destroyed. The corresponding decrease in serum PG I levels reflects the fall in chief cell mass (1 1 -1 3). PG II levels also diminish but to a lesser degree. Based on knowledge of precursor pathology, it is not surprising that both HP infection (a marker for chronic su- perficial gastnitis) and a low PG I level (a marker for atrophic gastnitis) increase gastric cancer risk. It is unknown, however, whether PG and HP are indicators of the same underlying process, independent risk factors, or risk factors that interact to jointly affect risk. In both asymptomatic patients and pa- tients with dyspepsia, HP-associated superficial gastritis has been linked with an increase, rather than a decrease in PG I; these levels return to normal with eradication of infection (1 4-1 6). However, HP infection in the presence of atrophic gastritis is associated with low PG I levels (17). on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Transcript of Helicobacter pylon, Pepsinogen, and Risk for Gastric ... · sion from normal stomach to malignancy...

Vol. 2, 46 1 -466, September/October 1993 Cancer Epidemiology, Biomarkers & Prevention 461
I The abbreviations used are: HP, Helicobacterpylori; PG I, pepsinogen I; PGII, pepsinogen II; OR, odds ratio; CI, confidence interval.
Helicobacter pylon, Pepsinogen, and Risk for GastricAdenocarc i noma
Julie Parsonnet,1 I. Michael Samloff, Lorene M. Nelson,Norman Orentreich, Joseph H. Vogelman, andGary D. Friedman2Division of Infectious Diseases and Geographic Medicine, Department of
Medicine II. P.1 and Division of Epidemiology, Department of HealthResearch and Policy Ii. P., L. M. NI, Stanford University, Stanford,California 94305; Division of Gastroenterology, Sepulveda Veterans
Administration Medical Center, Los Angeles, California II. M. 5.1;Orentreich Foundation for the Advancement of Science, Inc., Cold
Spring-on-Hudson, New York IN. 0., 1. H. V.1; and Division of Research,
Kaiser Permanente Medical Care Program, Oakland, California IC. D. F.l
Abstract
The objective of this project was to determine theassociation of Helicobacter pylon infection and serumpepsinogen levels on subsequent risk for gastricadenocarcinoma. This nested case-control study was setin a large health maintenance organization. Onehundred thirty-six cases of gastric adenocarcinoma and1 36 matched controls without adenocarcinoma from alarge cohort that had contributed serum in the 1960’swere studied. The presence of lgG against H. pylon hadpreviously been determined by enzyme-linkedimmunosorbent assay. Serum levels of pepsinogens I andII were ascertained by radioimmunoassay. In a sampleof subjects, the presence of antiparietal cell antibodieswas determined by immunofluorescent antibody assay(Nichols Laboratory). There were 98 cases ofadenocarcinoma of the antrum, body, or fundus (distalcancers) and 30 of the cardia or gastroesophagealjunction (proximal cancers). By univariate analysis,H. pylon infection [odds ratio (OR), 3.6; P < 0.001] andserum pepsinogen I < 50 ng/ml (OR = 2.9; P = 0.003)were both associated with development of distal cancer.In multivariate analysis, there was interaction betweenthe two variables; H. pylon in the absence of lowpepsinogen I was independently associated with cancer(OR, 2.4; P = 0.04) but low pepsinogen I in the absenceof H. pylon infection was not associated with cancer(OR, 0.8; P > 0.5). In combination, however, H. pyloninfection and a low pepsinogen I were associated with amarked increase in the risk of developing distalmalignancy (OR, 1 0.0; P = 0.08). Low serum pepsinogenI with H. pylon infection but not in its absence isassociated with a increased risk for distal gastric cancer.
Received 1/25/93; revised 4/5/93; accepted 4/5/93.
I To whom requestsfor reprints should be addressed, at HRP Building 2, Room
49, Stanford University, Stanford, CA 94305-5092. 1. P. is supported by an
Ortho Pharmaceuticals Young Investigator Award.2 G. D. F. is supported in part by Grant R35 CA49761 froni the National
Cancer Institute.
This suggests that infection rather than gastric atrophy isthe determining factor in cancer risk.
Introduction
Of cancer precursors, among the best described histopatho-logically are those preceding adenocarcinoma of the stom-ach. In prospective and cross-sectional studies, investigatorsin Europe and Latin America have documented the progres-sion from normal stomach to malignancy (1 , 2). The first ofthe precursor lesions, chronic superficial gastritis, appearsmany years before cancer is manifest. It is followed by atro-phic gastnitis, intestinal metaplasia, and dysplasia. While notall precursor stages are observed in any given individual,each successive step in the sequence increases the risk ofdeveloping this malignancy (1 , 3).
HP,t a bacterium that infects the mucosal lining of thestomach, causes the first of the precursor lesions, chronicsuperficial gastritis. Recently, three nested case-control stud-ies described an association between infection and subse-quent development of gastric cancer (4-6). Despite the dif-ferent populations evaluated (Japanese-American men inHawaii, men in Great Britain, and men and women in Cali-fomnia), the investigators reported remarkably similar results;infection with H. py!ori was associated with a 3-6-fold in-crease in the risk of developing gastric cancer.
Serum levels of pepsinogens, the proenzymes for thedigestive enzyme pepsin, have also been associated withincreased gastric cancer risk (7-9). Two immunochemicallydistinct classes of pepsinogens have been identified: PG I,which is produced in fundic mucous neck cells and in chiefcells of the gastric glands, and PG II, which is produced insimilar cells and in pylonic gland cells in the antrum (1 0). Inatrophic gastnitis, the gastric glands have been destroyed.The corresponding decrease in serum PG I levels reflects thefall in chief cell mass (1 1 -1 3). PG II levels also diminish butto a lesser degree.
Based on knowledge of precursor pathology, it is notsurprising that both HP infection (a marker for chronic su-perficial gastnitis) and a low PG I level (a marker for atrophicgastnitis) increase gastric cancer risk. It is unknown, however,whether PG and HP are indicators of the same underlyingprocess, independent risk factors, or risk factors that interactto jointly affect risk. In both asymptomatic patients and pa-tients with dyspepsia, HP-associated superficial gastritis hasbeen linked with an increase, rather than a decrease in PG I;these levels return to normal with eradication of infection(1 4-1 6). However, HP infection in the presence of atrophicgastritis is associated with low PG I levels (17).
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

462 Helicobacter pylon, Pepsinogen, and Gastric Adenocarcinoma
Table 1 Matched odds ratios for the associa tion of gastric cancer with Helicobacter py Ion IgG, pepsinogen I, and pepsinogen 2 by Iocation of tumor
Cases ControlsMatched
.odds ratio
95 /� CI P value
Distal adenocarcinomas (n = 98)
“I” with H. pylon lgG 85.7 62.2 3.6 (1 .7-7.4) <0.001
Median PG I (ng/ml( 71.4 78.5 0.003
‘5, with PG I <50 ng/mI 39.8 18.4 2.9 (1.5-5.8) 0.002
Median PG II )nWml) 5.8 6.0 0.2
Median ratio PG I/PG II 9.4 13.5 0.01
Proximal adenocarcinomas (n = 30)
“3, with H. pylon IgG 56.7 63.3 0.8 (0.3-2.0) 0.6
Median PG I )ng/ml) 85.9 78.1 0.6
% with PG I < 50 ngJml 20.0 6.7 5.0 (0.6-42.8) 0.09
Median PG II )npjml( 4.1 5.2 0.4
Median ratio PG I/PG II 14.8 16.7 0.6
To better understand the nature of the relationship be-tween infection, atrophy and cancer, we evaluated serumpepsinogen I and II levels in subjects from a recently reportednested case-control study of HP and gastric cancer (6).
Materials and Methods
Subject Selection. The 1 36 case-control pairs in this inves-tigation had previously been studied in a nested case-controlstudy of HP and gastric cancer (6). The pairs had been se-lected from a cohort of 1 28,992 persons who had providedserum as part of a multiphasic health evaluation between1964 and 1969. Pathological specimens and records fromcohort members who developed gastric cancer subsequentto their multiphasic examination (case subjects) had beenreviewed and tumors had been classified by histologicaltype and site within the stomach. Each case had beenmatched by a 5-year birth cohort, gender, mace, and site anddate of serum collection (same month and year) to one co-hort member (control subject) who had not developed can-cem in the time up to and including the year of the diagnosisof the case.
Serological Assays. Serum samples had been maintained infrozen storage at the Omentreich Foundation for the Ad-vancement of Science, Inc. (1 8). All sena from cases andcontrols had been previously evaluated for anti-HP lgG byserum enzyme-linked immunosombent assay as described(6). This assay has a sensitivity of 91% and a specificity of98% for active gastric infection. An additional 0.5 ml ofstored serum from each case and control was tested by ma-dioimmunoassay for PG I and PG II as previously described(19).
All sera with low PG I levels that were also negative forH. py!ori lgG (n = 9) were tested for antipanietal cell anti-bodies (courtesy of Nichols Institute Laboratory, San JuanCapistrano). Also tested for antipamietal cell antibodies wererandom samples of case and control sera with either: (a) lowPG I values and HP seropositivity (n = 1 5); or (b) normal PGI values and HP seronegativity (n = 18). Tested samples werediluted 1 :8 and 1 :32 in FTA hemagglutination buffer, pH 7.2(Becton Dickinson). Dilutions were overlaid on mouse stom-ach kidney (Sanofi Diagnostics Pasteur) and/or mouse storn-ach (Scimedx) slides. After a 30-mm incubation, the slideswere rinsed and washed in buffer for 1 0 mm, and the bufferwas changed after a 5-mm interval. Polyvalent fluomesceinisothiocyanate conjugate (lNCStar), at an appropriate dilu-
tion, was added to each well and incubated 30 mm. The
slides were rinsed and washed as above and read under afluorescent microscope for fluorescence of panietal cells. Atiter at a dilution greater than 1 :8 was considered positive.A titer of 1 :8 was considered equivocal.
For all assays, serological analysis was done withoutknowledge of the case-control status of the subject.
Statistical Analysis. Because adenocancinomas of the distalstomach (antnum and fundus) have a different pathogenesisthan tumors of the proximal stomach (cardia and gastnoe-sophageal junction), the distal and proximal cancer siteswere analyzed separately (20). The two histological types ofgastric adenocarcinoma, the intestinal and diffuse types,were analyzed in both combined and separate analyses (21).
PG I was considered both as a continuous variable andas a categorical variable. Strata for PG I included: <50 ng/ml; 50 to <75 ng/rnl; 75 to <1 00 ng/ml; 1 00 to <1 25 ng/ml;and �1 25 ng/ml. For the purpose of this study, a low PG Iwas defined as a level less than 50 ng/ml. This cutoff waschosen because it represented the lowest quartile of PG I inthe study population and it had previously been establishedas a cutoff for low PG I in normal, healthy adults (10).
Data were entered and analyzed with Epilnfo (Centersfor Disease Control, Atlanta, GA), Egret (Statisucs and Epi-demiology Research Corporation, Seattle, WA), and SPSSPC� (Statistical Package for the Social Sciences, Inc., Chi-cago, IL) computer programs. For dichotomous variables,odds ratios were determined as the ratio of discordant pairsand statistical significance was tested by the McNemammethod (22, 23). For categorical variables with more thantwo levels and for multivamiate analysis, odds ratios weredetermined by conditional logistic regression (24). Statisticaltests of the regression estimates were based on the � ap-proxirnation for the likelihood ratio statistic with confidenceintervals determined by Wald’s test. Interaction terms wereincluded to examine the joint association of risk factors onthe odds of developing gastric cancer. Comparison of me-dian values of continuous variables were determined usingWilcoxon rank sum test for matched data.
ResultsBanked serum samples from both members of the matchedcase-control pair were available for 1 29 (94.8%) of the 136pairs. From one control, a PG I level could not be obtained;this pair was excluded from analysis. From the remaining
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

0.2
Cancer Epidemiology, Biomarkers & Prevention 463
Odds ratio20- �
10
5
2
I
0.5 -
*
.1�
<50 50-75 75-100
Pepsinogen I level (ng/ml)
100-125 >125
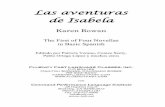
Fig. 1. Odds ratio for increased distal cancer risk by serum level of serum pepsinogen I. Five dummy variables were created. The odds ratio for cancer associated
with a pepsinogen I greater than 1 25 ng/ml was set at 1 .0. There was an large increase in risk associated with a pepsinogen level less than 50 ng/ml. PepsinogenI less than 50 ng/mI increased risk of cancer 4-fold when compared to levels of 1 25 ng/ml.
1 28 matched pairs, three cases lacked sufficient serum forthe PG II assay and only PG I levels were analyzed. Theevaluated pairs included 98 distal adenocamcinomas and 30proximal adenocarcinomas. Serum PG II levels were verylow in most sena, possibly reflecting instability of this zy-mogen in sena stored for more than 20 years. Because therewas no reason to suspect that storage affected serum PG IIlevels of cases and controls differently, the PG II data wereanalyzed as planned despite the unusually low values.
Cases and controls were very closely matched with me-spect to age (median age in cases and controls, 53.6), sex(28.1 % female in both cases and controls), and mace (white,78.1 0/; African-American, 1 9.5%; Asian, 2.3% in both casesand controls). For cases, the median interval between serumdonation and development of cancer was 1 5 years (range,1-24 years).
As we previously reported, HP was associated with de-veloprnent of distal but not proximal adenocarcinomas(Table 1) (6). Low PG I levels were also linked with devel-opment of distal but not proximal tumors. PG Il levels werenot linked with malignancy at any site although the abnon-mally low PG II values in our study population may haveobscured a true association (Table 1 ). The ratio of PG I to PGII, a frequently reported marker for cancer risk (9, 11, 16),was lower in cases than controls. In our population, thisappeared to be attributable to differences in PG I betweencases and controls.
Intesti nal and d iffuse-type tu moms were both associatedwith HP [OR, 3.0 (95#{176}hCl, 1 .3-6.7) and OR, 8.0 (95% CI,
1 .0-64.0), respectivelyl and PG 1 [OR, 2.8 (95% Cl 1 .3-6.0)
and OR, 3.5 (95% Cl 0.7-16.9), respectivelyl. Because the
histological types were similarly associated with the twoprincipal study risk factors, the remaining analyses of distalmalignancies combine the two tumor types.
A PG I level of less than 50 ng/ml was associated witha large increase in distal cancer risk when compared to alevel �125 ng/ml (OR, 3.8; 95% CI 1.0-13.5; Fig. 1).Intermediate levels of PG I (between 50 ng/ml and 1 25 ng/ml) were not significantly associated with increased risk ofdistal gastric carcinoma. PG I levels less than 50 ng/ml wereassociated with a 5-fold increased proximal cancer (Table 1).With the small sample size, this finding was not statistically
significant.Among distal cancer cases, PG I levels tended to be
lower in those with HP antibodies than in those without HPantibodies (Table 2). A level of PG I less than 50 ng/ml wassignificantly associated with infection. In controls, PG I 1ev-els tended to be higher in those with HPthan in those withoutalthough this finding was not significant. PG II levels ap-peamed to reflect HP antibody status since levels were in-creased in both cases and controls with HP antibodies whencompared to cases and controls without HP antibodies. ThePG I/PG II ratio was lower in HP senopositive subjects (bothcases and controls) than in semonegative subjects. The num-ben of subjects was too small in the proximal cancer groupto identify an association between HP and pepsinogens.
In conditional logistic regression models of distal can-cer pairs, there was no evidence ofconfounding between HPand a low PG I level; when both variables were assessedtogether, the odds ratios for distal cancer (OR, 3.5 for HPinfection; OR, 2.9 for PG I < SOng/mI) did not differ from theunadjusted odds ratios presented in Table 1 . Assessment of
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

464 f’Ielicobacter pylon, Pepsinogen, and Gastric Adenocarcinoma
Tab le 2 Pepsinogen Ievels (ng/mI) in cases a nd controls by Helic obacter pylon infecti on status
Cases Controls
With HP Without HP P value9j With HP Without HP P value”
Distal cancer
Median PG I
% with PG I <50
Median PG II”
Median PG I/PG II”
84
59.0
44.0
6.2
8.9
14
75.6
14.3
4.4
17.3
0.07
0.04
0.16
0.01
61
89.1
18.0
6.5
12.4
37
72.3
18.9
4.5
15.9
0.11
0.9
0.005
0.04
Proximal cancer
Median PG I
% with PG I <50
Median PG II
Median PG I/PG II
17
90.0
23.5
4.1
13.0
13
80.5
15.4
3.9
15.8
0.5
0.6
0.8
0.6
19
76.9
10.5
5.2
18.5
11
87.8
0
7.0
12.9
0.3
0.5
0.5
0.7
“ Tested by Wilcoxon Rank Sum Two Sample Test for PG I, PG II, and PG I/PG II ratio and tested by x2 for PG <50.
1, Excludes three cases from whom insufficient serum precluded PG II assay.
the joint effect of HP and PG I, however, revealed evidenceof an interaction between these risk factors (Table 3). Theodds ratio for cancer in HP-infected subjects with normal PGI levels compared to uninfected subjects with normal PG Ilevels was 2.4, (P 0.04). The odds ratio for cancer in HP-infected subjects with low PG I level was 4-fold higher, 10.0(P = 0.08). In the absence of HP infection, a low PG I levelwas not associated with later development of malignancy.
The joint effects of HP infection and low PG I level werealso assessed for subgroups formed by age, tumor type, andinterval from serum collection to cancer diagnosis (Table 3).Although the subgroups for these analyses were too small totest for interaction meaningfully, the joint effect of low PG
and HP infection remained consistent throughout the sub-groups. In no subgroup was a low PG I a risk factor withoutevidence of HP infection. These patterns were similar for ageand interval subgroups within the intestinal-type tumor painsalthough power was diminished due to smaller sample size.The interaction between HP and a low PG I level was morepronounced in pairs 55 years and older than in pairs youngerthan 55 years bR, 14.3 compared with OR, 5.4(P= 0.08)1.In the olden pains, the median PG I level among infected
cases was 45 ng/ml compared to 92 ng/ml in uninfectedcases (P = 0.11 ). Furthermore, 52.0% of cases compared to1 2.2% ofcontmols demonstrated both HP infection and a PGI level less than 50 ng/ml. In younger subjects, the medianPG I in infected cases was 72 ng/ml compared to 70 in un-infected cases (not significant). Only 22.9% of cases and10.2% of controls had both a low PG I and HP infection.
The antipanietal cell antibodytitem assay yielded equivo-cal results (titer of 1 :8) in 5 (1 2%) of 42 subjects tested (4controls and 1 case). Of the remaining 37 subjects, 3 (8%)had antipanietal cell antibody titers greaten than 1 :32 (Table4). All three, two controls and one case, had very low levelsof PG I (values 11.3, 16.5, and 24.5 ng/ml, respectively).Antipamietal cell antibodies could account for 2 (25%) of 8low PG I values that occurred in the absence of HP infection.The overall prevalence ofantipanietal cell antibodies was toolow, however, to estimate any associations between pemni-cious anemia, H. py!ori, and gastric cancer.
Discussion
H. py!ori infection has been established to be a risk factor forcancer of the gastric fundus, body and antrurn (4-6). It me-mains uncertain, however, whether H. py!ori plays a part in
disease causation on only marks a predisposition to malig-nancy. The dominant hypothesis in gastric cancinogenesismaintains that gastric atrophy, not H. py!ori infection, is cniti-cal in disease pathogenesis (25). Atrophy of pamietal cellscauses hypochlorhydnia. The loss of acid is then thought toallow bacteria to overgrow in the gastric mucosa and trans-form nitrites to carcinogenic N-nitnosoamines. In this study,we examined the mole of H. py!ori infection in determining
cancer risk in patients with and without low serum levels ofPG I, a marker for atrophic gastnitis and achlorhydnia. H.py!ori was associated with increased risk for gastric cancer,independent of serum PG I level. Although low serum PG Iwas also linked to increased risk in the group as a whole, itwas not associated with cancer in the absence of H. py!ori
infection. This implies that infection-related inflammation,rather than gastric atrophy alone, may be the critical factorin disease pathogenesis. The presence of atrophy may mag-nify risk attributable to other factors but it does not in itself
determine risk.Theme are several ways to explain a joint effect of HP and
PG I level. The presence of atrophy may merely reflect se-verity of HP infection or the host response to it. Alternatively,
atrophy itself may be detrimental when HP is coexistent.Either is physiologically plausible. Chronic inflammation
has been linked to numerous malignancies including can-cems of the bladder, biliary tree, and colon. The rapid turn-
oven ofcells associated with HP infection and the productionof tissue oxidants by inflammatory cells both would favorcell mutation (26, 27). Furthermore, HP produces unease, anenzyme that splits urea into ammonia and carbon dioxide.Investigators have shown that adding low concentrations ofammonia to the drinking water of rats (similar to the expo-sure caused by HP unease) produces atrophy and promotesmalignant transformation (28, 29). Thus, by several mecha-nisms, HP has the potential to cause mutation and cancer
without invoking the additional detrimental impact of atmo-phy.
It is also physiologically plausible, however, that atro-phy and hypoacidity are themselves deleterious when corn-bined with infection. One potential explanation incorpo-mates the protective effect of vitamin C on gastric cancer risk(30). The normal stomach excretes ascorbic acid activelyinto its lumen where levels exceed those in the serum (31).In the setting of HP infection, ascorbic acid levels in gastricjuice fall sharply (32, 33). Because ascorbic acid prevents
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 465
Table 3 Univariate and adjusted odds ratio (95% confidence intervals) for the association of gastric cancers of the antrum and fundus (distal c
H. pylon and pepsinogen 1 by tumor type, interval from serum collection to diagnosis, and age at serum collection”ancers) with
Univariate OR OR (95% Cl) for joint effect of HP and PG IP for HP PG I
HP PG5O No HP and HP No HP HP and interactionn PGI�50 PGI�50 PGk5O PGk5O
.
P tor 3-wayinteraction
All distal cancers 98 3.6 2.9 1.0 2.4 0.8 10.0
(1.7-7.4) (1.5-5.8) 11.0-5.61 10.1-4.41 13.3-30.51 0.08 NA
Intestinal type tumor 72 3.0 2.8 1 .0 2.0 0.8 8.3
(1.3-6.7) (1.3-6.0) 10.8-5.11 10.1-4.81 12.4-28.01 0.11
Diffuse type tumor 26 8.0 3.5 1 .0 Insufficient sample size
(1 .0-64.0) (0.7-16.9)
NA
Interval < 15 years 50 2.6 2.3 1.0 1.8 0.5 6.8
(1.1-6.2) (0.9-6.1) 10.7-4.91 10.05-6.11 11.6-29.81 0.14
Interval � 15 years 48 7.0 3.6 1.0 4.6 1.2 19.7
(1.6-30.8) (1.4-9.7) 10.9-23.91 10.08-16.81 12.9-133.11 0.39
0.8
Age at serum collection 46 3.4 1 .4 1 .0 2.8 0.5 5.4
<55 years (1.3-9.2) (0.6-3.4) 10.9-8.11 10.05-5.71 11.3-23.41 0.33
Age at serum collection 47 3.0 6.3 1.0 1.6 1.2 14.3
�55 years (1.0-9.3) (1.9-21.4) 10.4-6.71 10.07-20.41 12.2-94.11 0.19
0.08
“ NS, not significant; NA, not applicable or not testable.
Table 4 Results of antiparietal cell antibody testing on 42 subjects by H.
pylon antibody status and level of pepsinogen I
HP antibody and Total n n n with APA” n testedPG I status in study tested Cases Controls
HP antibody negative, 9 9 1/2 1/6”low PG I
HP antibody positive, 48 15 0/4 1/8’low PG I
HP antibody negative, 42 18 0/3” 0/14normal or high PG I
Total 99 42 1/9 2/28
a APA, antiparietal cell antibodies.
b Excludes one control with a borderline antiparietal cell antibody titer of 1 :8.
C Excludes three controls with borderline antiparietal cell antibody titers.
d Excludes one case with borderline antiparietal cell antibody titer.
N-nitmosation while achlorhydnia favors it, the combinationof infection and achlorhydnia could markedly augment risk.
Although one might expect to see a gradual increase inrisk with increasing atrophy, we observed a marked incre-ment when PG I values fell below 50 ng/ml. In a previousstudy with shorter follow-up of cancer cases (9), 20 ng/mlwere used to define a low pepsinogen. In our group however,only 18 subjects (11 with distal adenocarcinoma) met thiscriterion, providing too few subjects for statistical analysis.Recent studies demonstrate that a PG I level less than 50ng/ml discriminates patients with moderate on severe atro-phy of the corpus from persons with less severe disease. Instudies from one of our laboratories (I. M. Samloff), a serumPG I less than 30 ng/rnl was 90% sensitive and 93% specificfor severe atrophic gastnitis involving the all or part of thecorpus (1 1 ). A value less than 50 ng/ml was 93% sensitivefor moderate or severe atrophy although specificity de-dined. In another study, all 1 71 patients with moderate tosevere corpus atrophy on gastric biopsy had levels of PG 1less than 50 ng/mI. None of 50 patients with normal stom-achs had levels this low (1 0). We conclude that, to augmentcancer risk, a major portion of gastric glands in the stomachneed to have been destroyed.
Based on the location of inflammation within the stom-ach, chronic superficial gastnitis has been divided into two
major types: (a) gastnitis involving the stomach corpus (withor without accompanying antral gastnitis); and (b) gastnitis
restricted to the antrum. Historically, corpus gastnitis hasbeen linked to gastric cancer. While some patient with con-pus disease have pernicious anemia, recent data support arole for H. py!ori in pathogenesis of corpus disease (1 6). Thegastnitis most typically associated with H. py!ori is antral.Peptic ulcer disease, a disease of hyperacidity and increasedpepsinogen, namely occurs in the absence of this chronic in-flammatory lesion. Recently, investigators documented the
sequelae of antral and corpus gastnitis oven a span of 30-34years (34). Corpus disease tended to gradually progress to-wards atrophy although the rate of transformation slows in
the elderly. In contrast, antral gastnitis tended to regress oven
time, particularly in the elderly.Our data indicate that persons who develop cancer are
likely to have corpus involvement with HP. Even in youngercases, HP infection was associated with a decrease rather
than an increase in PG I. This loss of PG I attests to significantcorpus involvement. Our controls, on the other hand, ap-
peamed to have the more typical antral response to infection.Pepsinogen levels nose. This is the effect most commonly
reported for H. py!ori (1 4, 1 5, 35) and is consistent with thelower risk of malignancy observed in persons with peptic
ulcer disease (6). Antipanietal cell antibodies were uncom-mon in our study group and we could not specifically assess
the association of pernicious anemia-related atrophy on ma-lignancy.
Investigators have previously reported that HP causedan increase in both serum PG I and PG II (14, 15). In ourstudy, an elevated PG II level did reflect infection status. Thisassociation was statistically significant despite the unexpect-edly low PG IIvalues obtained from the stored sena. In con-
trast, we found that HP infection could be associated withboth increases and decreases in PG I. In controls, serum PGI levels were higher in infected persons than in uninfectedpatients. The opposite was true for the cases, in whom HP
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

466 Helicobacter pylon, Pepsinogen, and Gastric Adenocarcinoma
infection was actually associated with decreased PG I. Thus,the differential effect of HP on PG I appeared to predict can-cen risk.
The classic preneoplastic progression from normalstomach through gastnitis, atrophy, and intestinal metaplasiato gastric cancer has described only for intestinal-type ma-lignancy. Diffuse disease is not thought to succeed the typi-cal preneoplastic lesions. A previous study of pepsinogenssupported this distinction: in a nested design similar to ours,intestinal but not diffuse cancer patients were found to havehad low levels of PG I years before the onset of disease (9).Our study did not corroborate this distinction. Diffuse andintestinal disease were similar in respect to pepsinogens andHP infection. It is possible that tumor types were histolog-ically misclassified, causing bias in our results. It is also pos-sible, however, that the distinctions between intestinal anddiffuse disease are less firm than was previously thought.
Gastric cancer remains one of the leading causes ofcancer death worldwide. These data support a 10-fold in-creased risk for cancer in persons with both HP infection anda PG I level less than 50 ng/rnI. In persons olden than 55years, the relative risk association with this combination iseven higher. If these findings are reproduced by other in-vestigatons, the joint effect of HP and PG I on distal cancerrisk could be exploited for cancer control purposes. For ex-ample, in high-risk populations, persons with both risk fac-tons could be targeted for more intensive screening proce-dunes (i.e., endoscopy or photofluomoscopy). Furthermore, ifHP eradication in patients with atrophy is found to reducecancer risk, HP treatment may be a mechanism for inter-vention in the premalignant process.
Acknowledgments
We would like to thank Margaret Lopez of Nichols Institute Laboratories andShufang Yang of Stanford University for their technical support in this inves-
tigation and Jennifer Kelsey and Nancy Durr for their review ofthe manuscript.
References
1 . Correa, P., Haenszel, W., Cuello, C., et al. Gastric precancerous processin a high risk population: cohort follow-up. Cancer Res., 65: 2078-2084,1990.
2. Correa, P, Cuello, C, Duque, E., et al. Gastric cancer in Colombia. Ill.Natural history of precursor lesions. J. NaIl. Cancer Inst., 57: 27-35, 1976.
3. Sipponen, P., Kekki, M., Haapakoski, J., et al. Gastric cancer risk in
chronic atrophic gastritis: statistical calculations on cross-sectional data. Can-
cer, 35: 173-177, 1985.
4. Nomura, A., Stemmermann, C. N., Chyou, P., et al. Helicobacterpyloriinfection and gastric carcinoma in a population of Japanese-Americans inHawaii. N. EngI. I. Med., 325: 1132-1136, 1991.
5. Forman, D., Newell, D. C., Fullerton, F. et al. Association between in-
ection with Helicobacter pylon and risk of gastric cancer: evidence from aprospective investigation. Br. Med. J., 302: 1 302, 1991.
6. Parsonnet, I., Friedman, C. D., Vandersteen, D. P., et aI. Helicobacterpyloriinfection andthe risk ofgastric carcinoma. N. EngI. J. Med., 325:1127-
1131, 1991.
7. Farinati, F., Di Mario, F., Plebani, M., et al. Pepsinogen A/pepsinogen C
or pepsinogen A multiplied by gastrin in the diagnosis of gastric cancer. Ital.
I. Gastroenterol., 23: 1 94-1 96, 1991.
8. Nomura, A. M. Y., Stermmermann, C. N., and Samloff, I. M. Serum pep-
sinogen I as predictor of stomach cancer. Ann. Intern. Med., 93: 537-540,1980.
9. Stemmermam, C. M., Samloff, I. M., Normura, A. M. Y., and Heilbrun,L. K. Serum pepsinogens I and II and stomach cancer. Clin. Chim. Acta, 163:
191-198, 1987.
1 0. Samloff, I. M., and Liebman, W. M. Radioimmunoassay of group I pep-
sinogens in serum. Gastroenterology, 66: 494-502, 1974.
11 . Borch, K., Axelsson, K., Halgreen, H., et a!. The ratio of pepsinogen A
to pepsinogen C: a sensitive test for atrophic gastritis. Scand. I. Gastroenterol.,24:870-876, 1989.
12. Kekki, M., Samloff, I. M., Vans, K., and Ihamiki, 1. Serum pepsinogen
I and serum gastrin in the screening of severe atrophic gastritis. Scand. J.
Castroenterol., 186 (Suppl.): 117-123, 1991.
1 3. Vans, K., Kekki, M., Harkonen, M., etal. Serum pepsinogen I and serum
gastrin in the screening ofatrophic pan gastritis with high risk ofgastric cancer.
Scand. J. Castroenterol., 186 (Suppl.(: 117-123, 1991.
14. Fraser, A. C., Prewett, E. J., Pounder, R. E., and Samloff, I. M. Twenty-four
hour hyperpepsinogenaemia in Helicobacter pylon-positive subjects is abol-ished by eradication of the infection. AIim. Pharmacol. Ther., 6: 389-394,
1992.
1 5. Truesdale, R. A., Samloff, I. M., Chamberlain, C. E., et al. Serum pep-
sinogen I and II levels reflect the statues of Helicobacter pylon infection and
response to treatment. Castroenterology, 102: Al 80, 1992.
1 6. Veenendaal, R. A., Biemond, I., Pena, A. S., et al. Influence of age and
Helicobacter pylon infection on serum pepsinogens in healthy blood trans-fusion donors. Cut, 33:452-455, 1992.
1 7. Karnes, W. E., Samloff, I. M., Siurala, M., et al. Positive serum antibody
and negative tissue staining for Helicobacterpylori in subjects with atrophicbody gastritis. Gastroenterology, 101: 167-1 74, 1991.
1 8. Friedman, C. D., Blaner, W. S., Goodman, D. S., eta!. Serum retinol andretinol-binding protein levels do not predict subsequent lung cancer. Am. J.Epidemiol., 123:781-789, 1986.
1 9. Samloff, I. M. Pepsinogens I and II: purification from gastric mucosa andradioimmunoassay in serum. Castroenterology, 82: 26-33, 1982.
20. Ming, S. Adenocarcinoma and other malignant epithelial tumors of the
stomach. In: S. Ming and H. Goldman H. (eds.), Pathology of the Castroin-
testinal Tract. Philadelphia: WB Saunders, 584-61 7, 1992.
21 . Lauren, P. The two histological main types of gastric cancer: diffuse and
so-called intestinal type carcinoma. Acta Pathol. Microbiol. Scand., 64: 31-49, 1965.
22. Mantel, N., and Haenszel, W. Statistical aspects of the analysis of data
from retrospectivestudiesofdisease.J. NatI. Cancerlnst., 22:719-748, 1959.
23. Ejigou, A., and McHugh R. Estimation ofrelative risk from matched pairsin epidemiologic research. Biometrics, 33: 552-556, 1977.
24. Breslow, N. E., and Day, N. E. Statistical Methods in Cancer Research,Vol. I. The Analysis of Case-Control Studies, pp. 248-279. Lyon, France: In-
ternational Agency for Research on Cancer, 1980.
25. Correa, P., Haenszel, W., and Cuello, C., eta!. A model for gastric cancer
epidemiology. Lancet, ii: 50, 1975.
26. Tsujii, M., Kawano, S., and Ishigami, Y., et a!. Ammonia-produced byHelicobacter pylon accelerates cell proliferation rate of human gastric mu-cosa. New Orleans: Meeting Program for Digestive Disease Week, A-97 (Ab-
stract), 1991.
27. Jackson, J. H., Cajewski, E., and Schraufstatter, I. U., et a!. Damage to
the bases in DNA induced by stimulated human neutrophils. J. Clin. Invest.,
84: 164, 1989.
28. Tsujii, M., Kawano, S., Tsuji, S., et al. Ammonia: a possible promotor inHelicobacter pylon-related gastric carcinogenesis. San Francisco, CA: Meet-ing Program for Digestive Disease Week, A-41 6 (Abstract), 1992.
29. Kawano, S., Tsujii, M., Fusamoto, H., eta!. Chronic effect of intragastricammonia on gastric mucosal structures in rats. Dig. Dis. Sci., 102: 1881-1888, 1992.
30. Howson, C., Hiyama, T., and Wynder, E. The decline in gastric cancer:
epidemiology of an unplanned triumph. Epidemiol. Rev., 8: 1-27, 1986.
31. Sobola, C. M., Schorah, C. J., Sanderson, M., eta!. Ascorbic acid in thehuman stomach. Castroenterology, 97: 357-63, 1989.
32. Sobala, C. M., Crabtree, J. E., and Dixon, M. F., eta!. Acute He!icobacterpylon infection: clinical features, local and systemic immune response, gas-
tric mucosal histology and gastric juice ascorbic acid concentrations. Cut, 32:1415-1418, 1991.
33. Sobala, C. M., Pignatelli, B., Schorah, C. J., eta!. Levels ofnitrite, nitrate,N-nitroso compounds, ascorbic acid and total bile acids in gastric juice of
patients with and without precancerous conditions of the stomach. Carci-nogenesis (Lond.), 12: 193-198, 1991.
34. Ihamaki, T., Kekki, M., Sipponen, P., and Siurala, M. The sequelae and
course of chronic gastritis during a 30-to 34-year bioptic follow-up study.Scand. J. Castroenterol., 20: 485-491, 1985.
35. Sierra, R., Munoz, N., Pena, A. S., et al. Antibodies to Helicobacterpyloriand pepsinogen levels in children from Costa Rica: comparison of two
areas with different risks for stomach cancer. Cancer Epidemiol., Biomarkers& Prey., 1 : 449-54, 1992.
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1993;2:461-466. Cancer Epidemiol Biomarkers Prev J Parsonnet, I M Samloff, L M Nelson, et al. adenocarcinoma.Helicobacter pylori, pepsinogen, and risk for gastric
Updated version
http://cebp.aacrjournals.org/content/2/5/461
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/2/5/461To request permission to re-use all or part of this article, use this link
on April 2, 2020. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from