Fosfomicina i combinacionsi combinacions de Miro-23... · Fosfomicina y combinaciones 2.-Con...
39
Fosfomicina Fosfomicina i i combinacions combinacions XXII Jornades SCMIMC Castelldefels, 25-26 Octubre del 2013 XXII XXII Jornades Jornades SCMIMC SCMIMC Castelldefels Castelldefels , 25 , 25 - - 26 Octubre del 2013 26 Octubre del 2013 Dr. Jose M. Miro Servei de Malalties Infeccioses Hospital Clinic – IDIBAPS Universitat de Barcelona Barcelona Dr. Dr. Jose M. Jose M. Miro Miro Servei Servei de de Malalties Malalties Infeccioses Infeccioses Hospital Clinic Hospital Clinic – – IDIBAPS IDIBAPS Universitat Universitat de Barcelona de Barcelona Barcelona Barcelona Correu electrònic: [email protected] Correu Correu electrònic electrònic : : [email protected] [email protected]
Transcript of Fosfomicina i combinacionsi combinacions de Miro-23... · Fosfomicina y combinaciones 2.-Con...

Fosfomicina i combinacionsFosfomicinaFosfomicina i i combinacionscombinacions
XXII Jornades
SCMIMCCastelldefels, 25-26 Octubre del 2013
XXII XXII JornadesJornades
SCMIMCSCMIMCCastelldefelsCastelldefels, 25, 25--26 Octubre del 201326 Octubre del 2013
Dr. Jose M. MiroServei
de Malalties
Infeccioses
Hospital Clinic –
IDIBAPSUniversitat
de Barcelona
Barcelona
Dr. Dr. Jose M. Jose M. MiroMiroServeiServei
de de MalaltiesMalalties
InfecciosesInfeccioses
Hospital Clinic Hospital Clinic ––
IDIBAPSIDIBAPSUniversitatUniversitat
de Barcelonade Barcelona
BarcelonaBarcelona
Correu
electrònic: [email protected]
electrònicelectrònic: : [email protected]@ub.edu

Potential conflict of interestPotential conflict of interest
Dr. José
M Miró
has received honoraria for speaking or participating in Advisory Boards and/or research grants from
the following Pharmaceutical Companies:
Dr. José
M Miró
has received honoraria for speaking or participating in Advisory Boards and/or research grants from
the following Pharmaceutical Companies:
Glaxo
Smith Kline (GSK) Gilead Sciences Oxford ImmunotecPfizerRoche Theravance
Glaxo
Smith Kline (GSK) Gilead Sciences Oxford ImmunotecPfizerRoche Theravance
Abbott, Boehringer-IngelheimBristol-Myers Squibb Chiron Cubist MerckNovartis
Abbott, Boehringer-IngelheimBristol-Myers Squibb Chiron Cubist MerckNovartis

Fosfomicina y combinacionesFosfomicinaFosfomicina y combinacionesy combinaciones
1.-
Una de las siguientes afirmaciones del mecanismo de acción y la actividad in vitro de la fosfomicina
no es cierta
A.-
La fosfomicina
bloquea la síntesis de los precursores del
peptidoglucano. B.-
Es activa frente a S. aureus y S. epidermidis, incluyendo cepas
meticilín-resistentes. C.-
Es poco activa frente a Enterococcus spp.
D.-
Es activa frente a enterobacterias productoras de BLEEs.E.-
Es activa frente a Acinetobacter baumanii.
1.-
Una de las siguientes afirmaciones del mecanismo de acción y la actividad in vitro de la fosfomicina
no es cierta
A.-
La fosfomicina
bloquea la síntesis de los precursores del peptidoglucano.B.-
Es activa frente a S. aureus y S. epidermidis, incluyendo cepas
meticilín-resistentes.C.-
Es poco activa frente a Enterococcus spp.
D.-
Es activa frente a enterobacterias productoras de BLEEs.E.-
Es activa frente a Acinetobacter baumanii.

Chemical Structure of Fosfomycin
Fosfomycin, originally
named
phosphonomycin, was
discovered
in Spain
in 1969.It
is
a phosphonic
acid
derivative, with
an
extremely
low
molecular weight, and
shows
almost
no binding
to
proteins. Fosfomycin
is
a unique
antibiotic
that
is
chemically unrelated
to
any
other
known
antibacterial agent.
Its
empirical
formula is
C3
H7
O4
PC4
H11
NO3
Fosfomycin, originally
named
phosphonomycin, was
discovered
in Spain
in 1969.It
is
a phosphonic
acid
derivative, with
an
extremely
low
molecular weight, and
shows
almost
no binding
to
proteins. Fosfomycin
is
a unique
antibiotic
that
is
chemically unrelated
to
any
other
known
antibacterial agent.
Its
empirical
formula is
C3
H7
O4
PC4
H11
NO3

Fosfomycin
inhibits the enzyme MurA
(UDP-N-acetylglucosamine-3-enolpyruvyl transferase) that catalyses the addition of phosphoenolpyruvate
(PEP) to UDP-N-acetyl-glucosamine
(GlcNAc) to form UDP-N-acetyl-muramic
acid (UDP-MurNAc)
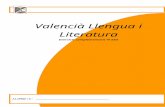
Actividad AntimicrobianaActividad AntimicrobianaActividad AntimicrobianaEfecto bactericida rápido sobre bacterias en fase de crecimiento. Es activa frente a estos microorganismos (CIM ≤32 mg/L):Gram
positivos
-
S. aureus y S. epidermidis (CIM<8 mg/L), incluyendo cepas productoras de betalactamasas
y meticilín-resistentes.
-
Menos activa frente Streptococcus y Enterococcus.Gram
negativos
-
E. coli, Salmonella, Shigella, Yersinia, Vibrio y Aeromonas (CIM90<8 mg/L).-
Más del 50% de cepas de Klebsiella, Enterobacter, Serratia, Proteus y el 20%
de P. aeruginosa tienen CIM 32-64 mg/L. Las bacterias anaerobias son sensibles.
→ Listeria monocitogenes, Acinetobacter baumanii y Bacteroides son resistentes.
Efecto bactericida rápido sobre bacterias en fase de crecimiento. Es activa frente a estos microorganismos (CIM ≤32 mg/L):Gram
positivos
-
S. aureus y S. epidermidis (CIM<8 mg/L), incluyendo cepas productoras de betalactamasas
y meticilín-resistentes.
-
Menos activa frente Streptococcus y Enterococcus.Gram
negativos
-
E. coli, Salmonella, Shigella, Yersinia, Vibrio y Aeromonas (CIM90<8 mg/L).-
Más del 50% de cepas de Klebsiella, Enterobacter, Serratia, Proteus y el 20%
de P. aeruginosa tienen CIM 32-64 mg/L.Las bacterias anaerobias son sensibles.→ Listeria monocitogenes, Acinetobacter baumanii y Bacteroides son resistentes.

Actividad de fosfomicina
frente a 200 aislados de S. aureus de pacientes con endocarditis del H. Clínic
de Barcelona (1997-2012)
Actividad de Actividad de fosfomicinafosfomicina
frente a 200 aislados de frente a 200 aislados de S. S. aureusaureus de de pacientes con endocarditis del H. pacientes con endocarditis del H. ClClíínicnic
de Barcelona (1997de Barcelona (1997--2012)2012)

Resistencia a la fosfomicinaResistencia a la Resistencia a la fosfomicinafosfomicinaAparecen mutantes resistentes con una frecuencia de 10-5.
La resistencia se debe a dos mecanismos:-
Mutaciones cromosómicas
en el mecanismo de transporte al
interior de la célula: sistemas GlpT
y/o UhpT -
Genes plasmídicos
(fosA, fosB, fosC, fosX) que codifican
metaloglutation
transferasas que inactivan a la fosfomicina. Este mecanismo es menos frecuente.
Debido a su mecanismo de acción, la resistencia cruzada con otros antibióticos es muy rara.
Aparecen mutantes resistentes con una frecuencia de 10-5.
La resistencia se debe a dos mecanismos:-
Mutaciones cromosómicas
en el mecanismo de transporte al
interior de la célula: sistemas GlpT
y/o UhpT-
Genes plasmídicos
(fosA, fosB, fosC, fosX) que codifican
metaloglutation
transferasas que inactivan a la fosfomicina. Este mecanismo es menos frecuente.
Debido a su mecanismo de acción, la resistencia cruzada con otros antibióticos es muy rara.
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739

Fosfomicina y combinacionesFosfomicinaFosfomicina y combinacionesy combinaciones
2.-
Con respecto a la farmacocinética y la posología de la fosfomicina, una de las siguientes afirmaciones no es cierta.
A.-
La dosis por vía intravenosa es de 100-300 mg/kg/día (8-24 g/día).
B.-
La dosis oral de fosfomicina-trometamol
es de 3 gramos en dosis única
C.-
Debe ajustarse la dosis en pacientes con insuficiencia renal.D.-
Debe ajustarse la dosis en pacientes con insuficiencia hepática.
E.-
El contenido en sodio de la formulación IV es elevado (330 mg/13,5 mEq/gramo).
2.-
Con respecto a la farmacocinética y la posología de la fosfomicina, una de las siguientes afirmaciones no es cierta.
A.-
La dosis por vía intravenosa es de 100-300 mg/kg/día (8-24 g/día).B.-
La dosis oral de fosfomicina-trometamol
es de 3 gramos en dosis
únicaC.-
Debe ajustarse la dosis en pacientes con insuficiencia renal.
D.-
Debe ajustarse la dosis en pacientes con insuficiencia hepática.E.-
El contenido en sodio de la formulación IV es elevado (330 mg/13,5
mEq/gramo).

Posología (adulto)PosologPosologíía (adulto)a (adulto)-
Oral*: sal calcíca
0’5-1 g/6h (biodisponibilidad 20%); trometamol
2-3 g en dosis única administrada a intérvalos
de 48-72 horas (biodisponibilidad del 40%). La administración con la comida puede disminuir la absorción.
-
Intravenosa: sal disódica, 100-300 -
máximo 400 mg/kg/día.
-
Contenido en sodio de los viales: 330 mg
(13,5 mEq) Na+/g
-
Insuficiencia hepática: sin cambios-
Insuficiencia renal: FG>40; sin cambios; FG 20-40: 4 g/12 h; FG
10-20: 4 g/d; FG<10: 2 g/d. Hemodiálisis/DP: dializa 80%/50%.
- Oral*: sal calcíca
0’5-1 g/6h (biodisponibilidad 20%); trometamol 2-3 g en dosis única administrada a intérvalos
de 48-72 horas
(biodisponibilidad del 40%). La administración con la comida puede disminuir la absorción.
-
Intravenosa: sal disódica, 100-300 -
máximo 400 mg/kg/día.-
Contenido en sodio de los viales: 330 mg
(13,5 mEq) Na+/g
-
Insuficiencia hepática: sin cambios-
Insuficiencia renal: FG>40; sin cambios; FG 20-40: 4 g/12 h; FG
10-20: 4 g/d; FG<10: 2 g/d. Hemodiálisis/DP: dializa 80%/50%.
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739* Solo para el tratamiento ITU.* Solo para el tratamiento ITU.

FarmacocinéticaFarmacocinFarmacocinééticatica-
Cmax: sal cálcica, 5-7 mg/L con 1-2 g oral; 30 mg/L con 3 g
trometamol
oral; y 90 mg/L con 2 g sal disódica
IV. - ABC24h
: 700 mg
x h/L con 12 g/día-
Fijación protéica: <5%
-
Vida media: 3 h (sal disódica); 5 h (sal cálcica); y 6 h (trometamol) -
Volumen de distribución: 0’3-0’5 L/kg
-
Metabolismo: No-
Eliminación: renal (FG), 85% (concentración urinaria pico >2.000
mg/L con 2-3 g de trometamol
durante >36 h a pesar de insuficiencia renal avanzada);
fecal 15%.
-
FC/FD: tiempo por encima CIM del 40-50% del intérvalo
entre dosis consecutivas.
-
Cmax: sal cálcica, 5-7 mg/L con 1-2 g oral; 30 mg/L con 3 g trometamol
oral; y 90 mg/L con 2 g sal disódica
IV.
- ABC24h
: 700 mg
x h/L con 12 g/día-
Fijación protéica: <5%
-
Vida media: 3 h (sal disódica); 5 h (sal cálcica); y 6 h (trometamol) -
Volumen de distribución: 0’3-0’5 L/kg
-
Metabolismo: No-
Eliminación: renal (FG), 85% (concentración urinaria pico >2.000
mg/L con 2-3 g de trometamol
durante >36 h a pesar de insuficiencia renal avanzada);
fecal 15%.
- FC/FD: tiempo por encima CIM del 40-50% del intérvalo
entre dosis consecutivas.
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739

Efectos secundariosEfectos secundariosEfectos secundarios→ Son poco frecuentes-
Intolerancia gastrointestinal (oral)
-
Diarrea-
Candidiasis
-
Hipersensibilidad-
Eosinofilia, trombocitosis
y hepatotoxicidad
-
Hipopotasemia-
Flebitis
-
Debido a su contenido en Na+
se recomienda utilizarla con precaución en pacientes con hipertensión, insuficiencia cardíaca, ascitis (cirróticos) o en hemodiálisis.
→ Son poco frecuentes-
Intolerancia gastrointestinal (oral)
-
Diarrea- Candidiasis- Hipersensibilidad- Eosinofilia, trombocitosis
y hepatotoxicidad
- Hipopotasemia- Flebitis-
Debido a su contenido en Na+
se recomienda utilizarla con
precaución en pacientes con hipertensión, insuficiencia cardíaca, ascitis (cirróticos) o en hemodiálisis.
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739; Florent
A et al. Int
J Antimicrob
Agents; 2011; 37: 82–92Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739; Florent
A et al. Int
J Antimicrob
Agents; 2011; 37: 82–92

Description
of
Adverse
Events
Associated
with
72 Courses of
Intravenous
Fosfomycin.
Description
of
Adverse
Events
Associated
with
72 Courses of
Intravenous
Fosfomycin.
Florent
A et al. Int
J Antimicrob
Agents; 2011; 37: 82–92Florent
A et al. Int
J Antimicrob
Agents; 2011; 37: 82–92
aGrade
1, 3 mmol/L≤K+
< 3.5 mmol/L; grade 3, 2.5 mmol/L≤K+
< 3mmol/L; and
grade 4, K+
< 2.5 mmol/L.bThese
adverse
events
were
attributed
to
fosfomycin
as all
differential
diagnoses
were
ruled
out (e.g. discontinuation
of
usual medication, atrial
fibrillation, myocardial
infarction, etc.).
aGrade
1, 3 mmol/L≤K+
< 3.5 mmol/L; grade 3, 2.5 mmol/L≤K+
< 3mmol/L; and
grade 4, K+
< 2.5 mmol/L.bThese
adverse
events
were
attributed
to
fosfomycin
as all
differential
diagnoses
were
ruled
out (e.g. discontinuation
of
usual medication, atrial
fibrillation, myocardial
infarction, etc.).
Aims of combination therapyAims of combination therapy
- To
look
for
synergy
and
greater
bactericidal
activity
- To
avoid
development
of
resistance
- To
decrease
individual doses
and
avoid
toxicity
- To
look
for
synergy
and
greater
bactericidal
activity
- To
avoid
development
of
resistance
- To
decrease
individual doses
and
avoid
toxicity
Fosfomycin, 100 mg/kg/d = 2 g/6h (70 kg)Fosfomycin, 100 mg/kg/d = 2 g/6h (70 kg)

Fosfomicina y combinacionesFosfomicinaFosfomicina y combinacionesy combinaciones3.-
La fosfomicina
no puede darse en monoterapia en infecciones sistémicas
estafilocócicas
ya que con rapidez aparecen mutantes resistentes. Por dicha razón, se recomienda su administración en combinación. Cual de las siguientes afirmaciones no es no es correcta frente a SARM:
A.-
La combinación con betalactámicos
(imipenem) es sinérgica en
células planctónicas B.-
La combinación con betalactámicos
(imipenem) es sinérgica en el
biofilm C.-
La combinación con daptomicina
es sinérgica en células planctónicas.
D.-
La combinación con daptomicina
es sinérgica en el biofilm.E.-
La combinación con rifampicina es sinérgica solo en el modelo de
biofilm.
3.-
La fosfomicina
no puede darse en monoterapia en infecciones sistémicas estafilocócicas
ya que con rapidez aparecen mutantes resistentes. Por dicha
razón, se recomienda su administración en combinación. Cual de las siguientes afirmaciones no es no es correcta frente a SARM:
A.-
La combinación con betalactámicos
(imipenem) es sinérgica en células planctónicasB.-
La combinación con betalactámicos
(imipenem) es sinérgica en el
biofilmC.-
La combinación con daptomicina
es sinérgica en células planctónicas.
D.-
La combinación con daptomicina
es sinérgica en el biofilm.E.-
La combinación con rifampicina es sinérgica solo en el modelo de
biofilm.
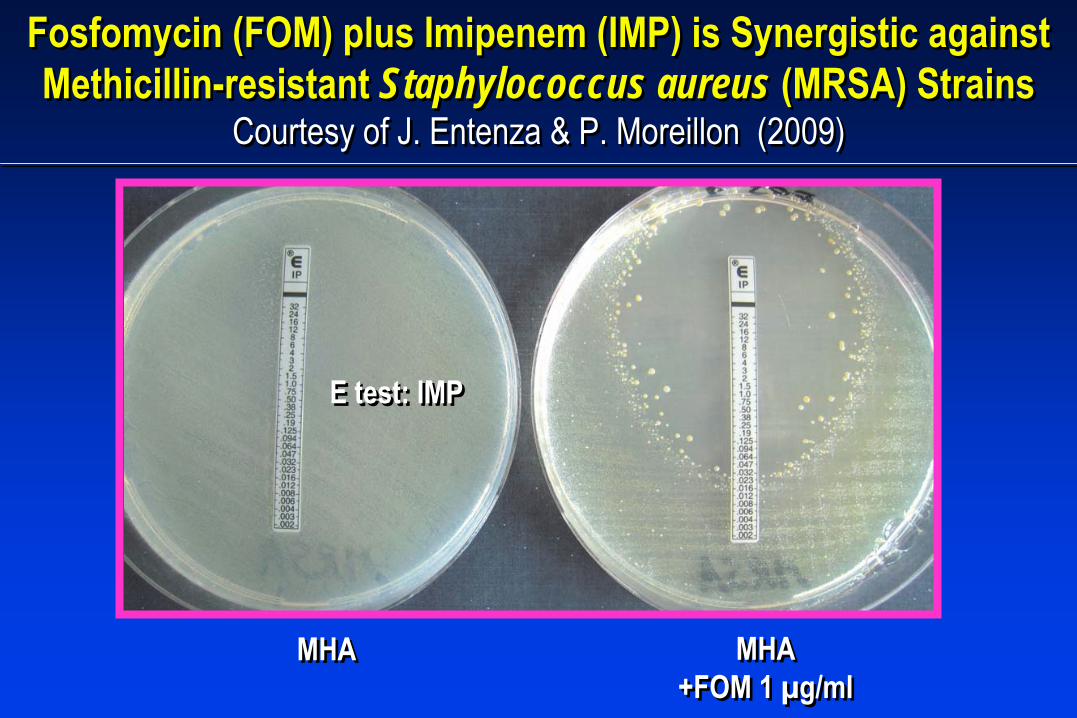
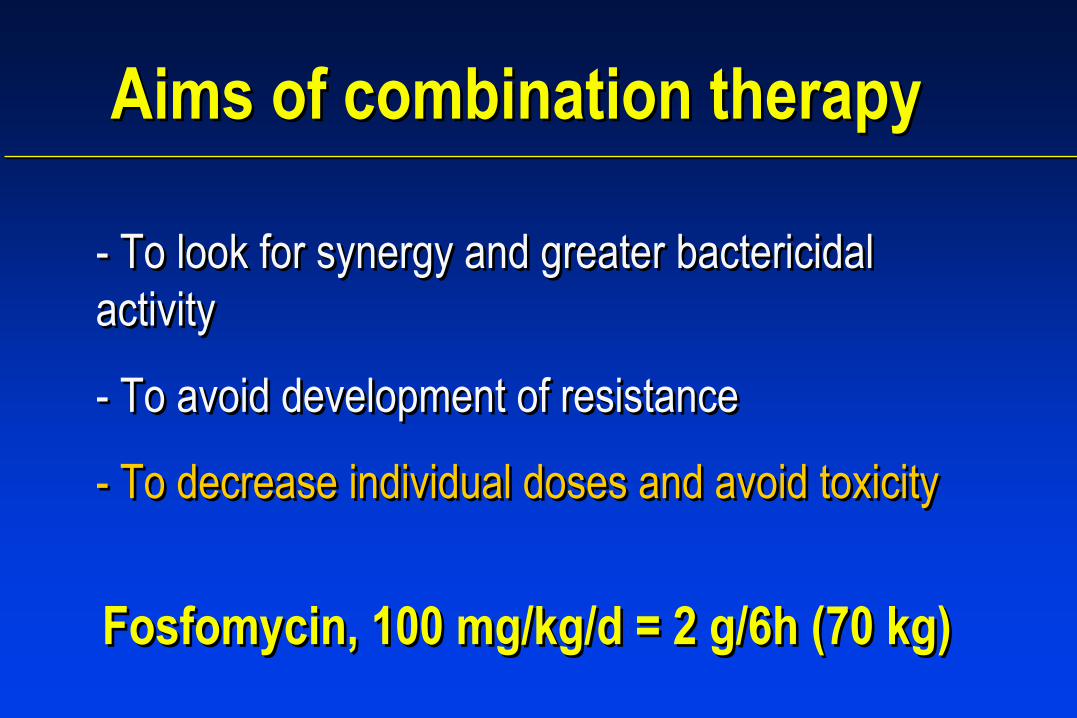
MHAMHA MHA+FOM 1 µg/ml
MHA+FOM 1 µg/ml
Fosfomycin
(FOM) plus Imipenem
(IMP)
is Synergistic against Methicillin-resistant Staphylococcus aureus (MRSA) Strains
Courtesy of J. Entenza
& P. Moreillon (2009)
Fosfomycin
(FOM) plus Imipenem
(IMP)
is Synergistic against Methicillin-resistant Staphylococcus aureus (MRSA) Strains
Courtesy of J. Entenza
& P. Moreillon (2009)
E test: IMPE test: IMP
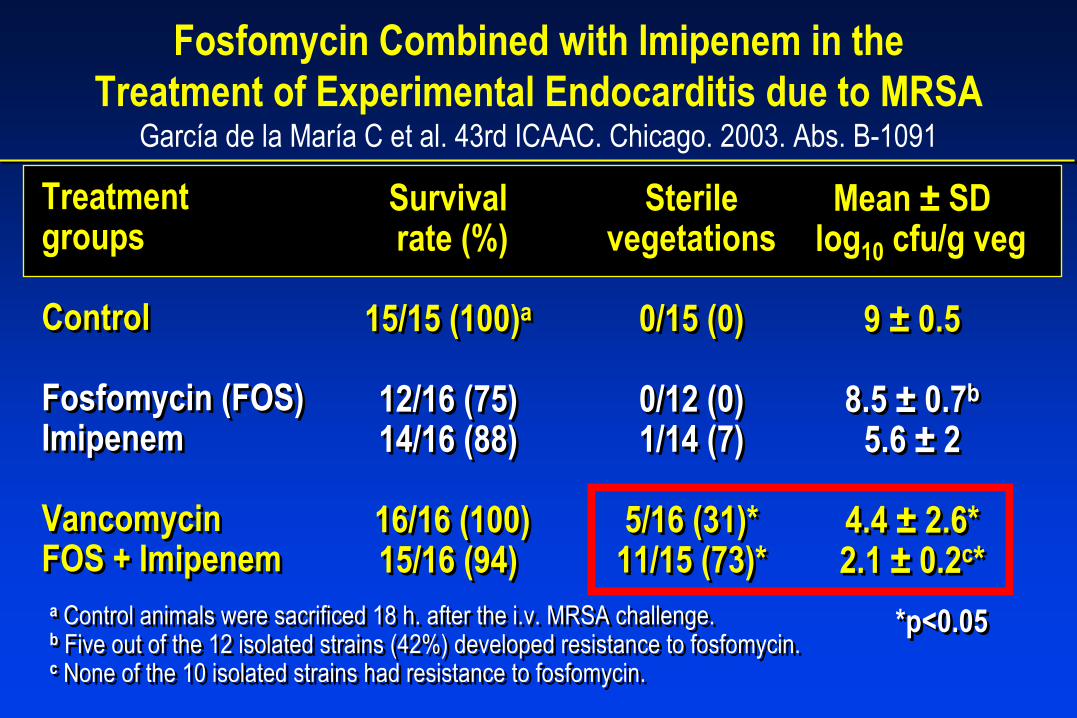
Treatmentgroups
Control
Fosfomycin
(FOS)Imipenem
VancomycinFOS + Imipenem
Treatmentgroups
Control
Fosfomycin
(FOS)Imipenem
VancomycinFOS + Imipenem
Mean ±
SDlog10
cfu/g
veg
9 ±
0.5
8.5 ±
0.7b
5.6 ±
2
4.4 ±
2.6*2.1 ±
0.2c*
Mean ±
SDlog10
cfu/g
veg
9 ±
0.5
8.5 ±
0.7b
5.6 ±
2
4.4 ±
2.6*2.1 ±
0.2c*
Sterile vegetations
0/15 (0)
0/12 (0)1/14 (7)
5/16 (31)*11/15 (73)*
Sterile vegetations
0/15 (0)
0/12 (0)1/14 (7)
5/16 (31)*11/15 (73)*
Survivalrate (%)
15/15 (100)a
12/16 (75)14/16 (88)
16/16 (100)15/16 (94)
Survivalrate (%)
15/15 (100)a
12/16 (75)14/16 (88)
16/16 (100)15/16 (94)
a
Control animals
were
sacrificed
18 h. after
the
i.v. MRSA challenge.b
Five
out of
the
12 isolated
strains
(42%) developed
resistance
to
fosfomycin. c
None
of
the
10 isolated
strains
had
resistance
to
fosfomycin.
a
Control animals
were
sacrificed
18 h. after
the
i.v. MRSA challenge.b
Five
out of
the
12 isolated
strains
(42%) developed
resistance
to
fosfomycin. c
None
of
the
10 isolated
strains
had
resistance
to
fosfomycin.
*p<0.05*p<0.05
Fosfomycin
Combined with Imipenem
in the Treatment of Experimental Endocarditis
due to MRSA
García
de la María
C et al. 43rd ICAAC. Chicago. 2003. Abs. B-1091

Synergy of the Combination of Fosfomycin
(FOS) and Imipenem
(IMP) Against MRSA and GISA is due to Decreased Synthesis of PBP1, PPB2
(but not PBP2a) and PBP3.del Rio A, Entenza
J, Miro
JM et al. 49th ICAAC. 2009. San Francisco (USA)
MRSA MRSA+ FOS
PBP 1
MRSA+ IMP
MRSA+ FOS+IMP
PBP 2aPBP 2
Kda
100
81
Standard
GISA GISA+ FOS
PBP 1
GISA+ IMP
GISA+ FOS+IMP
PBP 2aPBP 2PBP 3
PBP 4
100
81
PBP 3
47 PBP 4
Kda

Patient
123456789
PatientPatient
1122334456789
BC+before
F+I(days)
21711929721
IE Relapse*IE Relapse**
BC+BC+beforebefore
F+IF+I((daysdays))
221711929721
IE Relapse*IE Relapse**
F+I (days)
42752020161421928
F+I F+I ((daysdays))
42752020161421928
BC at 72 hF+I
---------
BC at 72 hBC at 72 hF+IF+I
---------
F/U BC at 45 d end
F+I
----
(1)(2)(3)--
F/U BC at 45 d F/U BC at 45 d endend
F+IF+I
----
(1)(2)(3)--
Median (range): 11 (2-29) 20 (9-75)
*3 weeks
V. **1 week
V AN + 3 weeks
DAP (6mg/Kg)
Median (range): 11 (2-29) 20 (9-75)
*3 weeks
V. **1 week
V AN + 3 weeks
DAP (6mg/Kg)(1) Dead
at 30 days
after
the
end
F+I Rx, BC-
(2) Dead
at 22 days
after
the
end
F+I Rx, BC-(3) Dead
at 14 days
after
the
end
F+I Rx, BC-
(1) Dead
at 30 days
after
the
end
F+I Rx, BC-(2) Dead
at 22 days
after
the
end
F+I Rx, BC-
(3) Dead
at 14 days
after
the
end
F+I Rx, BC-
Fosfomycin
+ Imipenem
for the Treatment of MRSA NV IE Failing Vancomycin
or Daptomycin
Therapy: Preliminary Results of a CT
del Río A, Gasch
O, Moreno A et al. Manuscript in preparation
FosfomycinFosfomycin
+ + ImipenemImipenem
for the Treatment of MRSA NV IE Failing for the Treatment of MRSA NV IE Failing VancomycinVancomycin
or or DaptomycinDaptomycin
Therapy: Preliminary Results of a CTTherapy: Preliminary Results of a CT
del Rdel Ríío A, o A, GaschGasch
O, Moreno A et al. Manuscript in preparationO, Moreno A et al. Manuscript in preparation

Fosfomycin
+ Imipenem
for the Treatment of MRSA NV IE Failing Vancomycin
or Daptomycin
Therapy: Preliminary Results of a CT
del Río A, Gasch
O, Moreno A et al. Manuscript in preparation
FosfomycinFosfomycin
+ + ImipenemImipenem
for the Treatment of MRSA NV IE Failing for the Treatment of MRSA NV IE Failing VancomycinVancomycin
or or DaptomycinDaptomycin
Therapy: Preliminary Results of a CTTherapy: Preliminary Results of a CT
del Rdel Ríío A, o A, GaschGasch
O, Moreno A et al. Manuscript in preparationO, Moreno A et al. Manuscript in preparation
No relapses

•
Recruitment: 2009-10; 12 weeks of F/U.•
Drugs adjusted to renal failure
•
Susceptible to study drugs (Excluded patients with strains with a Vanco
MIC = 2 mg/L)•
End points: To remain bacteremic
at 7 days, Toxicity, Resistance, Surgery and Mortality.
•
Recruitment: 2009-10; 12 weeks of F/U.•
Drugs adjusted to renal failure
•
Susceptible to study drugs (Excluded patients with strains with a Vanco
MIC = 2 mg/L)•
End points: To remain bacteremic
at 7 days, Toxicity, Resistance, Surgery and Mortality.
Multicenter, Randomized (1:1) Open-label Clinical Trial
Vancomycin
(≥
30 mg/kg)Cmin
≥
15 mg/L
FOS (2 g/ 6h, IV)+ IMI (1 g/6h, IV)
Evaluation of the efficacy and safety of fosfomycin
(FOS) plus imipenem
(IMI) for the treatment of MRSA IE (FOSIMI Trial)
FIS EC08/00190 -
PI: Dr. Asuncion Moreno
MRSA IE(N=50)

Daptomycin
(DAP) plus Fosfomycin
(FOM) is Synergistic against Methicillin-susceptible (MSSA) and Methicillin-
resistant Staphylococcus aureus (MRSA) Strains Miro
JM et al. Antimicrob
Agents
Chemother. 2012; 56:4511-5
Daptomycin
(DAP) plus Fosfomycin
(FOM) is Synergistic against Methicillin-susceptible (MSSA) and Methicillin-
resistant Staphylococcus aureus (MRSA) StrainsMiro
JM et al. Antimicrob
Agents
Chemother. 2012; 56:4511-5
MSSA (N=6) MRSA (N=6)
Two
patients
with
complicated
MRSA NV IE and
one
patient
with
MSSA PVE were succesfully
treated
with
daptomycin
(10 mg/kg) plus fosfomycin
(2 g/6h).
Two
patients
with
complicated
MRSA NV IE and
one
patient
with
MSSA PVE were succesfully
treated
with
daptomycin
(10 mg/kg) plus fosfomycin
(2 g/6h).

The Combination of Daptomycin
plus Fosfomycin
has Synergistic, Potent, and Rapid Bactericidal Activity against
MRSA in a Rabbit Model of EE Miro
JM et al. ECCMID, Barcelona 2014 (submitted)
The Combination of Daptomycin
plus Fosfomycin
has Synergistic, Potent, and Rapid Bactericidal Activity against
MRSA in a Rabbit Model of EEMiro
JM et al. ECCMID, Barcelona 2014 (submitted)

Daptomycin and β-lactams (Nafcillin)•
DAP + NAF as salvage regimen–
7 cases with persistent MRSA bacteremia
(7-22 days) –
DAP used as 2nd
line agent in all
– Only one case with DAP non-susceptibility
– Bacteremia
cleared with nafcillin
(NAF)
• Why?–
Increased daptomycin
membrane
binding with addition of NAF. –
Nafcillin
led to a reduction in the
net positive surface charge.
• DAP + NAF as salvage regimen–
7 cases with persistent MRSA bacteremia
(7-22 days)–
DAP used as 2nd
line agent in all
– Only one case with DAP non-susceptibility
– Bacteremia
cleared with nafcillin
(NAF)
• Why?–
Increased daptomycin
membrane
binding with addition of NAF.–
Nafcillin
led to a reduction in the
net positive surface charge.
Dhand
A et al. Clin
Infect Dis. 2011;53:158-163.Dhand
A et al. Clin
Infect Dis. 2011;53:158-163.
DAP (green) binding with &without NAF (yellow)
Slide courtesy of Vance Fowler, Duke University. Durham, NCSlide courtesy of Vance Fowler, Duke University. Durham, NC

Daptomycin
In Vitro Activity
against
MRSA
Is
Enhanced
by Cycloserine in a Mechanism
Associated
with
a Decrease
in Cell
Surface
Charge
Gasch
O et al. Antimicrobial
Agents
and
Chemotherapy
2013 (in press).
Daptomycin
In Vitro Activity
against
MRSA
Is
Enhanced
by Cycloserine in a Mechanism
Associated
with
a Decrease
in Cell
Surface
Charge
Gasch
O et al. Antimicrobial
Agents
and
Chemotherapy
2013 (in press).

Fosfomycin-Daptomycin
& Other
Fosfomycin
Combinations
asAlternative
Therapies
in Experimental Foreign-Body Infection
by MRSA
Garrigos
C et al. Antimicrobial
Agents
and
Chemotherapy
2013; 57:606–610
Fosfomycin-Daptomycin
& Other
Fosfomycin
Combinations
asAlternative
Therapies
in Experimental Foreign-Body Infection
by MRSA
Garrigos
C et al. Antimicrobial
Agents
and
Chemotherapy
2013; 57:606–610

Fosfomicina y combinacionesFosfomicinaFosfomicina y combinacionesy combinaciones
4.-
Cual de las siguientes afirmaciones respecto al tratamiento con fosfomicina
de las infecciones urinarias no es correcta
A.-
Debe administrarse siempre en combinación.B.-
Puede utilizarse la formulación oral.
C.-
Es útil para tratar infecciones por K. pneumoniae resistentes a las carbapenemasas. D.-
Es útil para tratar infecciones por Enterococcus faecium resistente a
la vancomicina. E.-
Es útil para el tratamiento de infecciones por E. coli productoras de
BLEEs.
4.-
Cual de las siguientes afirmaciones respecto al tratamiento con fosfomicina
de las infecciones urinarias no es correcta
A.-
Debe administrarse siempre en combinación.B.-
Puede utilizarse la formulación oral.
C.-
Es útil para tratar infecciones por K. pneumoniae resistentes a las carbapenemasas. D.-
Es útil para tratar infecciones por Enterococcus faecium resistente a
la vancomicina. E.-
Es útil para el tratamiento de infecciones por E. coli productoras de
BLEEs.

Uso Clínico en Infecciones por BGN y EFUso ClUso Clíínico en Infecciones por BGN y EFnico en Infecciones por BGN y EFTratamiento oral de ITU no complicadas, recurrentes (monoterapia)*-
E. coli incluyendo cepas productoras de BLEE
-
Enterococcus spp
incluyendo VRE→ Dosis única = 7-10 días nitrofurantoina, TMP-SMX, norfloxacina
Tratamiento intravenoso (siempre en combinación)-
Enterococcus
spp. resistente vancomicina (VRE)
-
Bacterias Gram
negativas multirresistentes: Enterobacterias productoras de BLEE, Klebsiella pneumoniae resistente carbapenemes; Pseudomonas aeruginosa**
Tratamiento oral de ITU no complicadas, recurrentes (monoterapia)*-
E. coli incluyendo cepas productoras de BLEE
- Enterococcus spp
incluyendo VRE→ Dosis única = 7-10 días nitrofurantoina, TMP-SMX, norfloxacina
Tratamiento intravenoso (siempre en combinación)-
Enterococcus
spp. resistente vancomicina (VRE)
-
Bacterias Gram
negativas multirresistentes: Enterobacterias productoras de BLEE, Klebsiella pneumoniae resistente carbapenemes; Pseudomonas aeruginosa***Incluyendo embarazadas (puede emplearse embarazo (B) y lactancia); ** Efecto protector nefrotoxicidad
por aminoglucósidos
y colistina
(probablemente por estabilización de la membrana lisosomas.
*Incluyendo embarazadas (puede emplearse embarazo (B) y lactancia); ** Efecto protector nefrotoxicidad
por aminoglucósidos
y colistina
(probablemente por estabilización de la membrana lisosomas.
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739

Fosfomycin
Synergy
In Vitro with
Amoxicillin, Daptomycin, andLinezolid
against
Vancomycin-Resistant
Enterococcus faecium from
Renal Transplant
Patients
with
Infected
Urinary
Stents
Fosfomycin
Synergy
In Vitro with
Amoxicillin, Daptomycin, andLinezolid
against
Vancomycin-Resistant
Enterococcus faecium from
Renal Transplant
Patients
with
Infected
Urinary
Stents
Descourouez
JL et al. Antimicrob
Agents
Chemother. 2013; 57:1518–1520Descourouez
JL et al. Antimicrob
Agents
Chemother. 2013; 57:1518–1520

In vivo Activity
of
the
Combination
of
Daptomycin
and
FosfomycinAgainst
a Strain
of
Enterococcus faecalis with
High-Level
Gentamicin
Resistance
in the
Rat
Endocarditis Model
In vivo Activity
of
the
Combination
of
Daptomycin
and
FosfomycinAgainst
a Strain
of
Enterococcus faecalis with
High-Level
Gentamicin
Resistance
in the
Rat
Endocarditis Model
Rice LB et al. DMID. 1992Rice LB et al. DMID. 1992

Experience
with
Fosfomycin
for
Treatment
of
Urinary
Tract Infections
Due
to
Multidrug-Resistant
Organisms
Experience
with
Fosfomycin
for
Treatment
of
Urinary
Tract Infections
Due
to
Multidrug-Resistant
Organisms
Neuner
EA et al. Antimicrob
Agents
Chemother. 2012; 56:5744–5748Neuner
EA et al. Antimicrob
Agents
Chemother. 2012; 56:5744–5748

Synergistic
effect
between
fosfomycin
and
specific
other antimicrobial
agents
for
Gram
negative
bacterial strains
Synergistic
effect
between
fosfomycin
and
specific
other antimicrobial
agents
for
Gram
negative
bacterial strains
Kastoris
AC et al. Eur
J Clin
Pharmacol. 2010; 66:359–368Kastoris
AC et al. Eur
J Clin
Pharmacol. 2010; 66:359–368
Β-lactamQuinolonesAminoglicosides

Fosfomycin
for
the
treatment
of
MDR, including
ESBL producing Enterobacteriaceae
infections: a systematic
review
Fosfomycin
for
the
treatment
of
MDR, including
ESBL producing Enterobacteriaceae
infections: a systematic
review
Falagas
ME et al. Lancet Infect
Dis
2010; 10: 43–50Falagas
ME et al. Lancet Infect
Dis
2010; 10: 43–50
E. coli = 97%E. coli = 97%
Klebsiella = 81%Klebsiella = 81%
Clinical cure94%
Clinical cure94%

IV Fosfomycin
for
the
Treatment
of
Nosocomial
Infections
caused
byCarbapenem-resistant
Klebsiella pneumoniae in Critically
ill
Patients
IV Fosfomycin
for
the
Treatment
of
Nosocomial
Infections
caused
byCarbapenem-resistant
Klebsiella pneumoniae in Critically
ill
Patients
Michalopoulus
A et al. Clin
Microbiol Infect
2010; 16: 184–186Michalopoulus
A et al. Clin
Microbiol Infect
2010; 16: 184–186
Fosfomycin was given
in combination with:- Colistin
(6),
- Gentamicin (3), - Piperacillin/tazobactam
(1)
Mortality
= 18%

IV Fosfomycin for BSI
PhosphonicPhosphonic
broad spectrum antibiotic that acts by broad spectrum antibiotic that acts by inhibiting the initial step of cell wall synthesisinhibiting the initial step of cell wall synthesis Epoxide
ring
• Bactericidal, good PK/PD properties.• Low toxicity (risk of sodium overload)• Rapid emergence of resistance in monotherapy• Combination therapy is mandatory for BSI• Combinations with other antibiotic families are synergistic• Good activity in animal models of several ID• Encouraging results in BSI & IE by MRSA, EF and GNB
• Bactericidal, good PK/PD properties.• Low toxicity (risk of sodium overload)• Rapid emergence of resistance in monotherapy• Combination therapy is mandatory for BSI• Combinations with other antibiotic families are synergistic• Good activity in animal models of several ID• Encouraging results in BSI & IE by MRSA, EF and GNB
Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739Michalopoulos
AS et al. Int
J Infect
Dis. 2011; 15:e732-e739

Members of the Hosp. Clinic Cardiovascular Infections & Experimental Endocarditis
Working Group
Members of the Hosp. Clinic Cardiovascular Infections & Experimental Endocarditis
Working Group
InfectiousDiseases
JM PericasC. CerveraA. MorenoJM GatellJM Miró
InfectiousDiseases
JM PericasC. CerveraA. MorenoJM GatellJM Miró
ExperimentalEndocarditis
Lab.
C. García de la MaríaY. Armero
ExperimentalEndocarditis
Lab.
C. García de la MaríaY. Armero
CardiologyC. FalcesJC Paré
M. AzquetaM. SitgesM. Heras
CardiologyC. FalcesJC Paré
M. AzquetaM. SitgesM. Heras
Barcelona-
SpainBarcelona-
Spain
ExternalCollaborators
G.R. CoreyV. FowlerJ. Entenza
P. Moreillon
ExternalCollaborators
G.R. CoreyV. FowlerJ. Entenza
P. Moreillon
MicrobiologyF. MarcoM. Almela
J. Vila
MicrobiologyF. MarcoM. Almela
J. Vila
Cardiac Surgery
CA MestresR. Cartañá
S. NinotJL Pomar
Cardiac Surgery
CA MestresR. Cartañá
S. NinotJL Pomar
PathologyJ. RamírezT. Ribalta
PathologyJ. RamírezT. Ribalta
Other ServicesD. Soy
M. BrunetJ. Llopis
Other ServicesD. Soy
M. BrunetJ. Llopis



Greenwood D. Antimicrobial Greenwood D. Antimicrobial agentsagents. In Greenwood D et al (. In Greenwood D et al (EdsEds).).Medical Medical MicrobiologyMicrobiology. 16th Edition. . 16th Edition. EdinburghEdinburgh. Churchill Livingstone. 2002.. Churchill Livingstone. 2002.
Fosfomicina: mecanismo de acción.