Farmacología Cardiovascular SISTEMA CIRCULATORIO: FUNCIONES PRINCIPALES Transportar y distribuir...
74
Farmacología Cardiovascular
-
date post
20-Dec-2015 -
Category
Documents
-
view
220 -
download
0
Transcript of Farmacología Cardiovascular SISTEMA CIRCULATORIO: FUNCIONES PRINCIPALES Transportar y distribuir...

Farmacología Cardiovascular

SISTEMA CIRCULATORIO: FUNCIONES PRINCIPALES
• Transportar y distribuir sustancias esenciales a los tejidos
• Remover desechos metabólicos
• Ajustar la provisión de oxígeno y nutrientes en diferentes estados metabólicos
• Regulación de la temperatura corporal
• Comunicación humoral
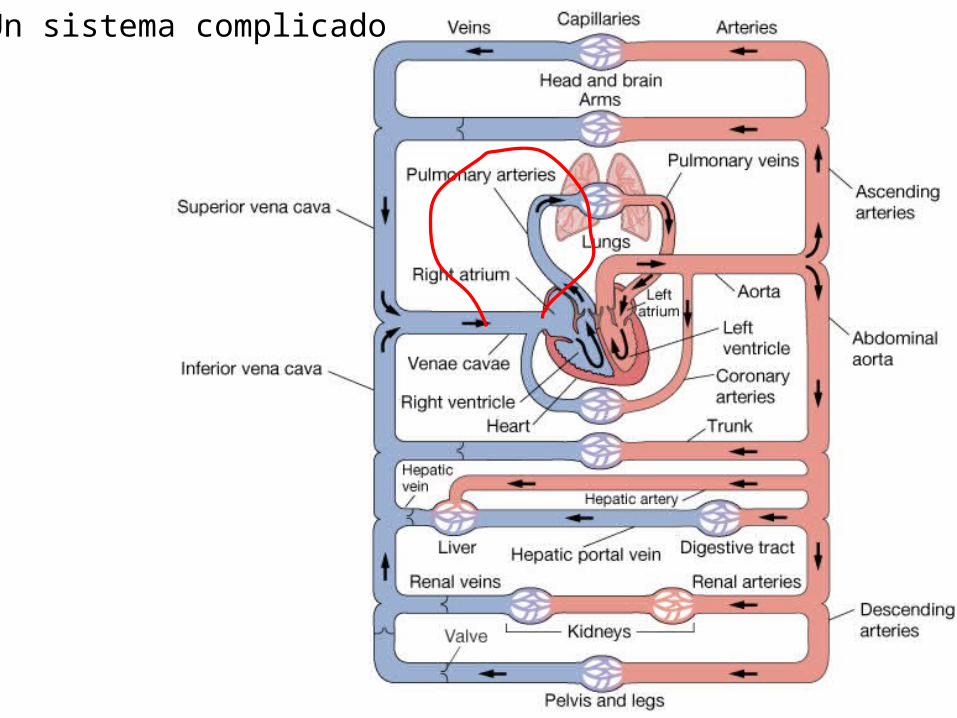
Un sistema complicado

Que se puede simplificar
SERIES AND
PARALLEL CIRCUITS


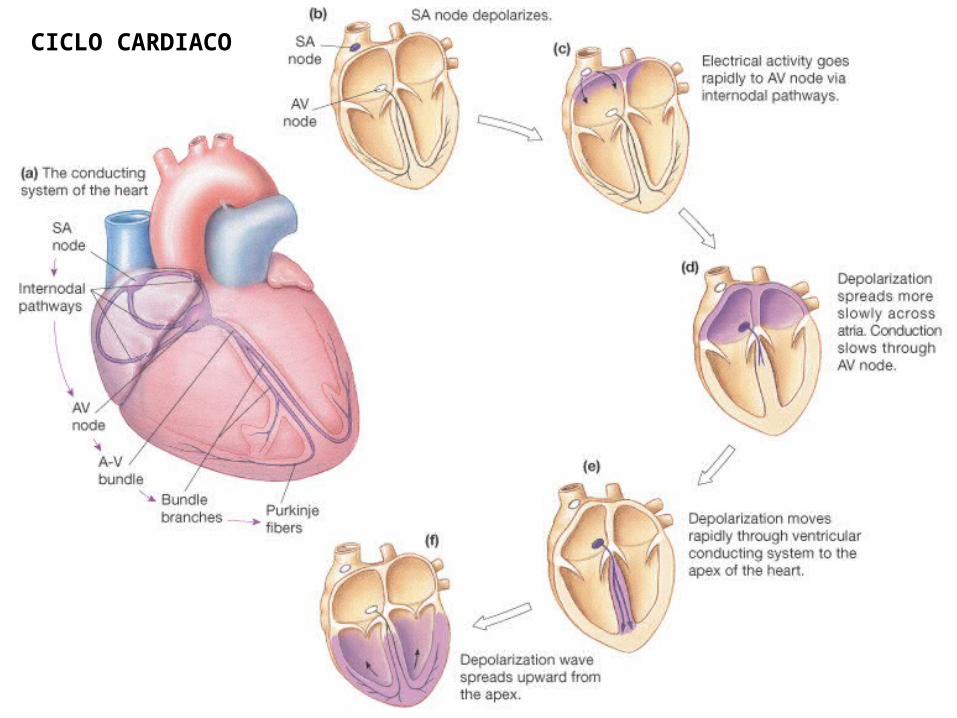
CICLO CARDIACO

Potencial de acción cardíacom
v
0
-80mv
mv
0
-80mv
mv
0
-80mv
ATRIUM VENTRICLE
SA NODE
time

Conductacias del PA cardíaco

Fast K closes Slow K opens
Fast K reopens
("Delayed rectifier")
Corrientes y PA cardíaco

Del PA al ECG




AV NODE AND AV BLOCKS
FOCUS ON N REGION
NORMAL
ECG
1ST DEGREE
PROLONGUED AVCONDUCTION TIME
2ND DEGREE
1/2 ATRIAL IMPULSES CONDUCTED TO VENTRICLES
3RD DEGREE
VAGAL MEDIATIONIN N REGION/COMPLETEBLOCK


• Cardiovascular disease is the major cause of death
• Cardiovascular function based on– Cardiac pumping ability
• Pace-making electrical signals• Force of contraction• Height of ventricle discharge pressure
– Integrity of vasculature• Presence of blockage• Muscular tone/structural integrity• Pressure drop needed to move blood to and through capillary
beds
– Blood volume/composition• Water, electrolyte, iron balances• Lipid and protein composition
ENFERMEDAD CARDÍACA

Patologías cardiovasculares que requieren farmacoterapia
• Hipertensión
• Arritmia
• Falla cardíaca
• Trastornos de flujo vascular

I. Background to Hypertension -Regulation of Blood Pressure
• Arterial blood pressure due to combination of cardiac output (CO) and total peripheral resistance (TPR)
• CO – regulated by heart rate and stroke volume (CO = HR x SV)
• TPR function of – Viscosity of blood (hematocrit)– Length of blood vessels– Blood vessel luminal diameter (especially precapillary
arterioles)
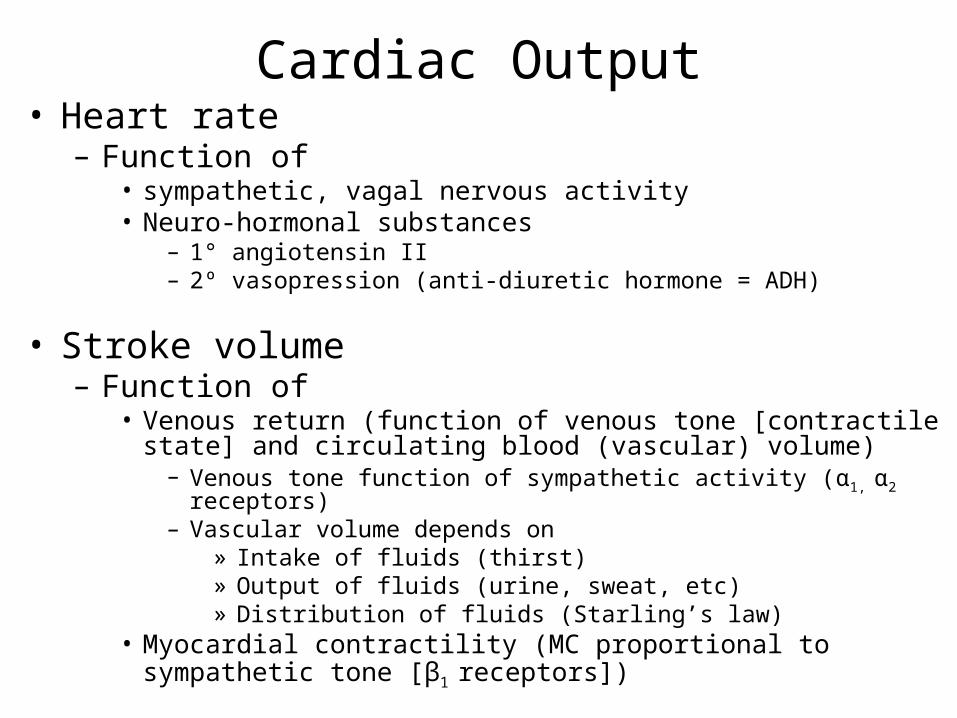
Cardiac Output• Heart rate
– Function of • sympathetic, vagal nervous activity• Neuro-hormonal substances
– 1° angiotensin II– 2º vasopression (anti-diuretic hormone = ADH)
• Stroke volume– Function of
• Venous return (function of venous tone [contractile state] and circulating blood (vascular) volume)
– Venous tone function of sympathetic activity (α1, α2 receptors)– Vascular volume depends on
» Intake of fluids (thirst)» Output of fluids (urine, sweat, etc)» Distribution of fluids (Starling’s law)
• Myocardial contractility (MC proportional to sympathetic tone [β1 receptors])

Characteristics of some adrenoceptors (sympathetic nerves)
α1 α2 β1 β2
Smooth muscle Arteries/
veins
constrict constrict/
dilate
dilate
Skeletal
muscle
dilate
Heart
Rate (increase)
Force of
contraction
increase
Tissues and effects receptors
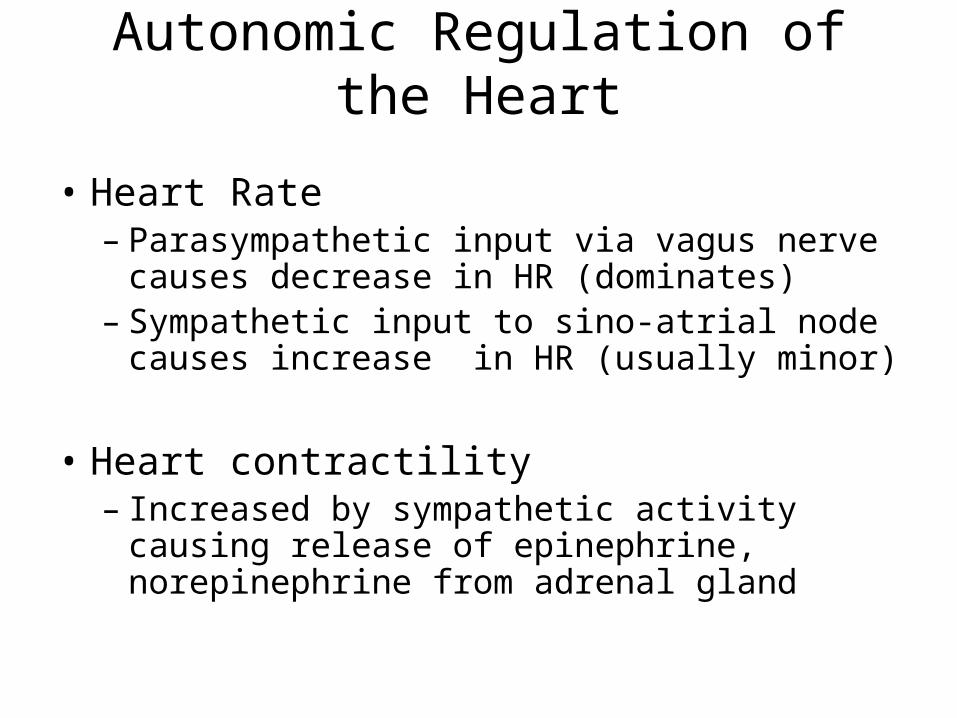
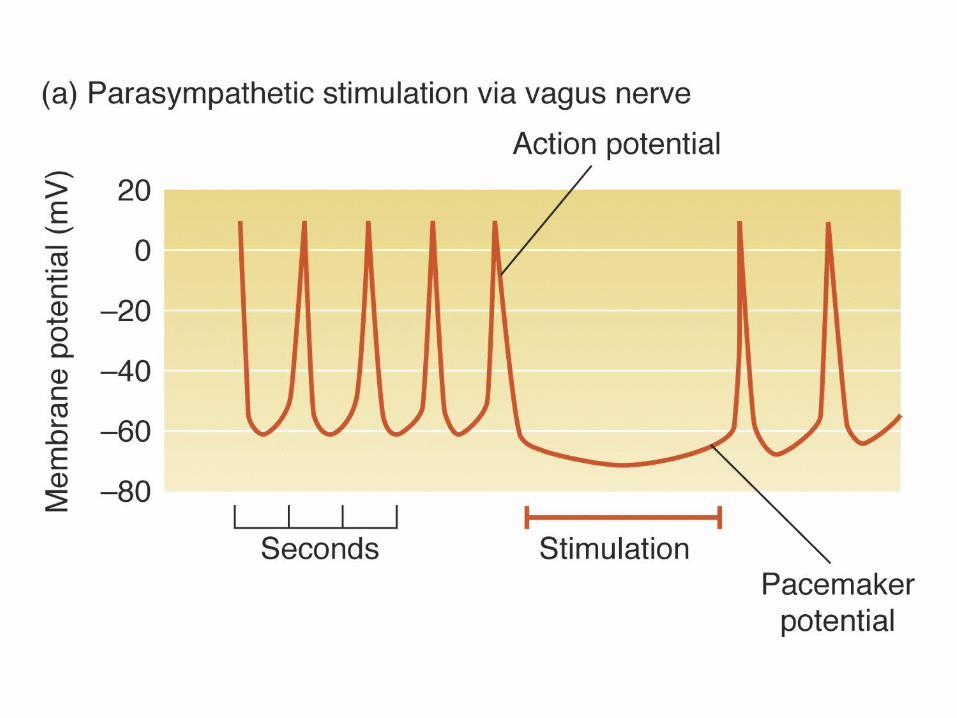
Autonomic Regulation of the Heart
• Heart Rate– Parasympathetic input via vagus nerve
causes decrease in HR (dominates) – Sympathetic input to sino-atrial node causes
increase in HR (usually minor)
• Heart contractility– Increased by sympathetic activity causing
release of epinephrine, norepinephrine from adrenal gland

Hipertensión

Antihypertensive Classes
• diuretics
• beta blockers
• angiotensin-converting enzyme (ACE) inhibitors
• calcium channel blockers
• vasodilators

Alpha1 Blockers
Stimulate alpha1 receptors -> hypertension
Block alpha1 receptors -> hypotension
• doxazosin (Cardura®)
• prazosin (Minipress®)
• terazosin (Hytrin®)
• doxazosin (Cardura®)
• prazosin (Minipress®)
• terazosin (Hytrin®)

Central Acting Adrenergics
• Stimulate alpha2 receptors – inhibit alpha1 stimulation
• hypotension
• clonidine (Catapress®)
• methyldopa (Aldomet®)
• clonidine (Catapress®)
• methyldopa (Aldomet®)

Peripheral Acting Adrenergics
• reserpine (Serpalan®)
• inhibits the release of NE
• diminishes NE stores
• leads to hypotension
• Prominent side effect of depression– also diminishes seratonin

Adrenergic Side Effects
• Common– dry mouth, drowsiness, sedation &
constipation– orthostatic hypotension
• Less common– headache, sleep disturbances, nausea, rash
& palpitations
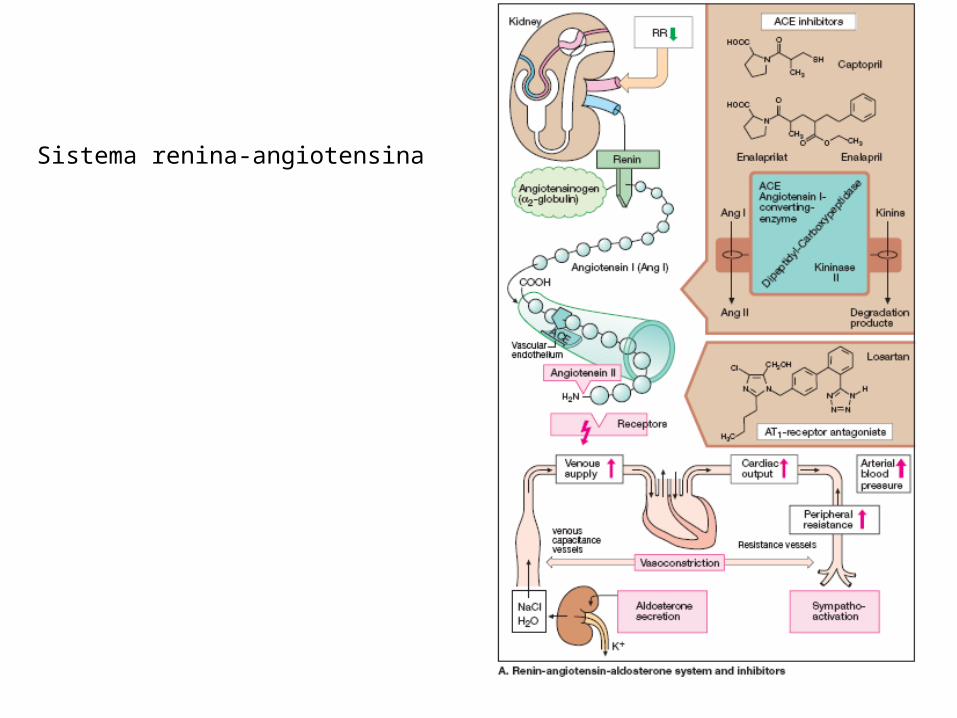
Sistema renina-angiotensina

Angiotensin I
ACE
Angiotensin II
1. potent vasoconstrictor
- increases BP
2. stimulates Aldosterone
- Na+ & H2O
reabsorbtion
ACE Inhibitors
.
RAAS

Renin-Angiotensin Aldosterone System
• Angiotensin II = vasoconstrictor• Constricts blood vessels & increases BP• Increases SVR or afterload• ACE-I blocks these effects decreasing SVR &
afterload

ACE Inhibitors
• Aldosterone secreted from adrenal glands
cause sodium & water reabsorption
• Increase blood volume
• Increase preload
• ACE-I blocks this and decreases preload

Angiotensin Converting Enzyme Inhibitors
• captopril (Capoten®)
• enalapril (Vasotec®)
• lisinopril (Prinivil® & Zestril®)
• quinapril (Accupril®)
• ramipril (Altace®)
• benazepril (Lotensin®)
• fosinopril (Monopril®)
Calcium Channel Blockers
• Used for:
• Angina
• Tachycardias
• Hypertension

Antagonistas de calcio como vasodilatadores
Calcium Channel Blockers
• diltiazem (Cardizem®)
• verapamil (Calan®, Isoptin®)
• nifedipine (Procardia®, Adalat®)

CCB Site of Action
diltiazem & verapamil
nifedipine (and otherdihydropyridines)

CCB Action
• diltiazem & verapamil
• decrease automaticity & conduction in SA & AV nodes
• decrease myocardial contractility
• decreased smooth muscle tone
• decreased PVR
• nifedipine
• decreased smooth muscle tone
• decreased PVR

Side Effects of CCBs
• Cardiovascular
• hypotension, palpitations & tachycardia
• Gastrointestinal
• constipation & nausea
• Other
• rash, flushing & peripheral edema
Diuretics
• Thiazides:
• chlorothiazide (Diuril®) & hydrochlorothiazide (HCTZ®,
HydroDIURIL®)
• Loop Diuretics
• furosemide (Lasix®), bumetanide (Bumex®)
• Potassium Sparing Diuretics
• spironolactone (Aldactone®)

Diuretic Site of Action
.
loop of Henle
proximaltubule
Distal tubule
Collecting duct

Mechanism
• Water follows Na+
• 20-25% of all Na+ is reabsorbed into the blood
stream in the loop of Henle
• 5-10% in distal tubule & 3% in collecting ducts
• If it can not be absorbed it is excreted with the
urine
Blood volume = preload !

Side Effects of Diuretics
• electrolyte losses [Na+ & K+ ]
• fluid losses [dehydration]
• myalgia
• N/V/D
• dizziness
• hyperglycemia

Vasodilators
• diazoxide [Hyperstat®]
• hydralazine [Apresoline®]
• minoxidil [Loniten®]
• sodium Nitroprusside [Nipride®]

Mechanism of Vasodilators
• Directly relaxes arteriole smooth muscle
• Decrease SVR = decrease afterload
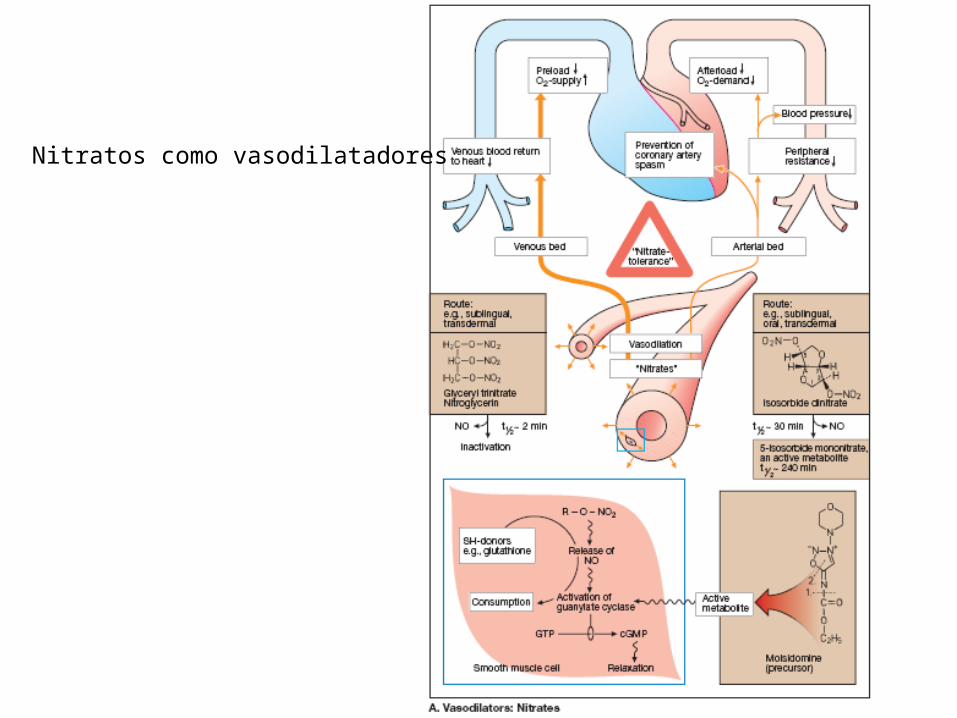
Nitratos como vasodilatadores

Side Effects of Vasodilators
• hydralazine (Apresoline®)– Reflex tachycardia
• sodium nitroprusside (Nipride®)– Cyanide toxicity in renal failure– CNS toxicity = agitation, hallucinations, etc.
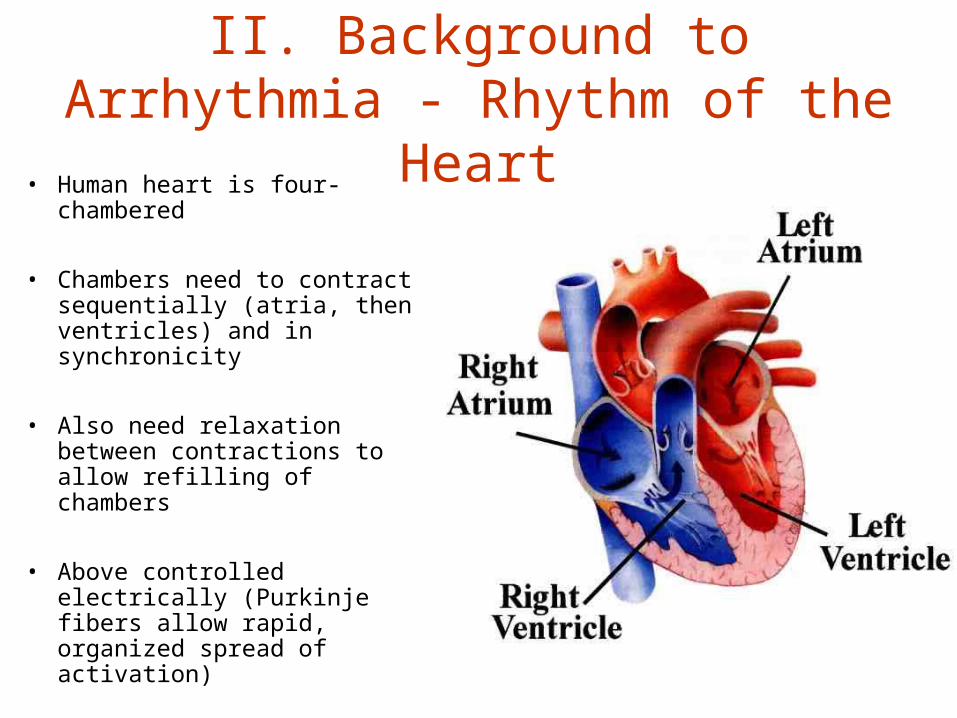
II. Background to Arrhythmia - Rhythm of the Heart
• Human heart is four-chambered
• Chambers need to contract sequentially (atria, then ventricles) and in synchronicity
• Also need relaxation between contractions to allow refilling of chambers
• Above controlled electrically (Purkinje fibers allow rapid, organized spread of activation)

Regulation of Heart Rate
– Primarily accomplished by sinoatrial node (SA)• Located on right atrium
• Receives autonomic input
• When stimulated, SA signals atrial contractile fibers atria depolarization and contraction (primes ventricles with blood)
– Depolarization picked up by atrioventricular node (AV node) depolarizes ventricles blood discharged to pulmonary artery and dorsal aorta eventually rest of body

Sequential Discharge of SA and AV nodes

Dysrhythmia Generation
• Abnormal conduction
• Analogies:– One way valve– Buggies stuck in
muddy roads

Antiarrítmicos: conducción cardíaca

Antiarrítmicos: bloqueo de canales de sodio
Warning!• All antidysrhythmics have arrythmogenic
properties
• In other words, they all can CAUSE dysrhythmias too!

Class I: Sodium Channel Blockers
• Decrease Na+ movement in phases 0 and 4
• Decreases rate of propagation (conduction) via tissue with fast potential (Purkinje)– Ignores those with slow potential (SA/AV)
• Indications: ventricular dysrhythmias

Class Ia Agents
• Slow conduction through ventricles
• Decrease repolarization rate– Widen QRS and QT
intervals• May promote
Torsades des Pointes!
• PDQ:– procainamide
(Pronestyl®)– disopyramide
(Norpace®)– qunidine – (Quinidex®)

Class Ib Agents
• Slow conduction through ventricles
• Increase rate of repolarization
• Reduce automaticity– Effective for ectopic
foci
• May have other uses
• LTMD:– lidocaine (Xylocaine®)– tocainide (Tonocard®)– mexiletine (Mexitil®)– phenytoin (Dilantin®)
Class Ic Agents
• Slow conduction through ventricles, atria & conduction system
• Decrease repolarization rate
• Decrease contractility• Rare last chance drug
• flecainide (Tambocor®)
• propafenone (Rythmol®)
Class II: Beta Blockers
• Beta1 receptors in heart attached to Ca++ channels– Gradual Ca++ influx responsible for
automaticity
• Beta1 blockade decreases Ca++ influx– Effects similar to Class IV (Ca++ channel
blockers)
• Limited # approved for tachycardias
Class II: Beta Blockers
• propranolol (Inderal®)
• acebutolol (Sectral®)
• esmolol (Brevibloc®)

Class III: Potassium Channel Blockers
• Decreases K+ efflux during repolarization• Prolongs repolarization• Extends effective refractory period• Prototype: bretyllium tosylate (Bretylol®)
– Initial norepi discharge may cause temporary hypertension/tachycardia
– Subsequent norepi depletion may cause hypotension

Class IV: Calcium Channel Blockers
• Similar effect as ß blockers
• Decrease SA/AV automaticity
• Decrease AV conductivity• Useful in breaking
reentrant circuit• Prime side effect:
hypotension & bradycardia
• verapamil (Calan®)• diltiazem (Cardizem®)
• Note: nifedipine doesn’t work on heart

III. Background to Congestive Heart Failure Maintenance of Normal Heart Function
• Normal cardiac output needed to adequately perfuse peripheral organs– Provide O2, nutrients, etc– Remove CO2, metabolic wastes, etc– Maintain fluid flow from capillaries into interstitium and back into venous
system if flow reduced or pressure increased in venous system build up of interstitial fluid = edema
• Because CO is a function of– Heart Rate – determined by pacemaker cells in the sinoatrial node– Stroke volume – determined by fill rate and contractile force– Atrial/ventricular/valvular coordination
Any negative change on above can lead to inadequate perfusion and development of the syndrome of heart failure

FALLA CARDÍACACAUSES: Impairment of electrical activity
Muscle damageValvular defectsCardiomyopathiesResult of drugs or toxins
PROBLEM: Maintaining circulation with a weak pump( Cardiac output & cardiac reserve; RAP)
SOLUTIONS: Sympathetic tone via baroreceptor reflex - Heart rate and contractility
-Venoconstriction ( MCP)-Vasoconstriction ( Arterial BP)
Fluid retention ( MCP)-Capillary fluid shift-ADH-Renin-angiotensin-aldosterone

Glicósidos:Efectos cardíacos

IV. Background to Reduced Vascular Blood Flow: Blood Vessel Anatomy and Function
• Arterial blood vessels– Smooth muscle (slow, steady contraction)– elastic tissue (stretch on systole, recoil on diastole)– Contain about 10% of blood volume– Arterioles have sphincters which regulate 70% of blood pressure
• Venous blood vessels– Highly distensible, some contractility– Contain over 50% of blood volume
• Capillaries– Tiny but contain greatest cross-sectional area to allow high exchange rate– Contain precapillary sphincters to regulate blood flow– 5% of blood volume
All vasculature under ANS and humeral control
Misc. Agents
• adenosine (Adenocard®)– Decreases Ca++ influx & increases K+ efflux
via 2nd messenger pathway• Hyperpolarization of membrane• Decreased conduction velocity via slow potentials• No effect on fast potentials
• Profound side effects possible (but short-lived)
Misc. Agents
• Cardiac Glycocides
• digoxin (Lanoxin®)– Inhibits NaKATP pump– Increases intracellular Ca++
• via Na+-Ca++ exchange pump
– Increases contractility– Decreases AV conduction velocity

Fármacos con acción cardíaca
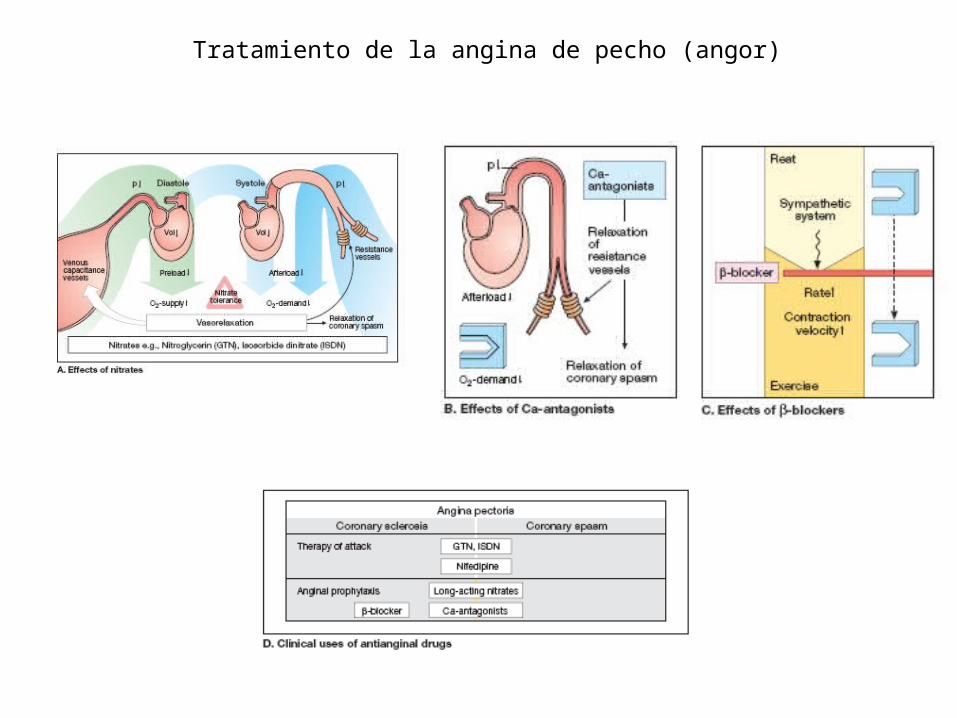
Tratamiento de la angina de pecho (angor)

Tratamiento del infarto agudo de miocardio
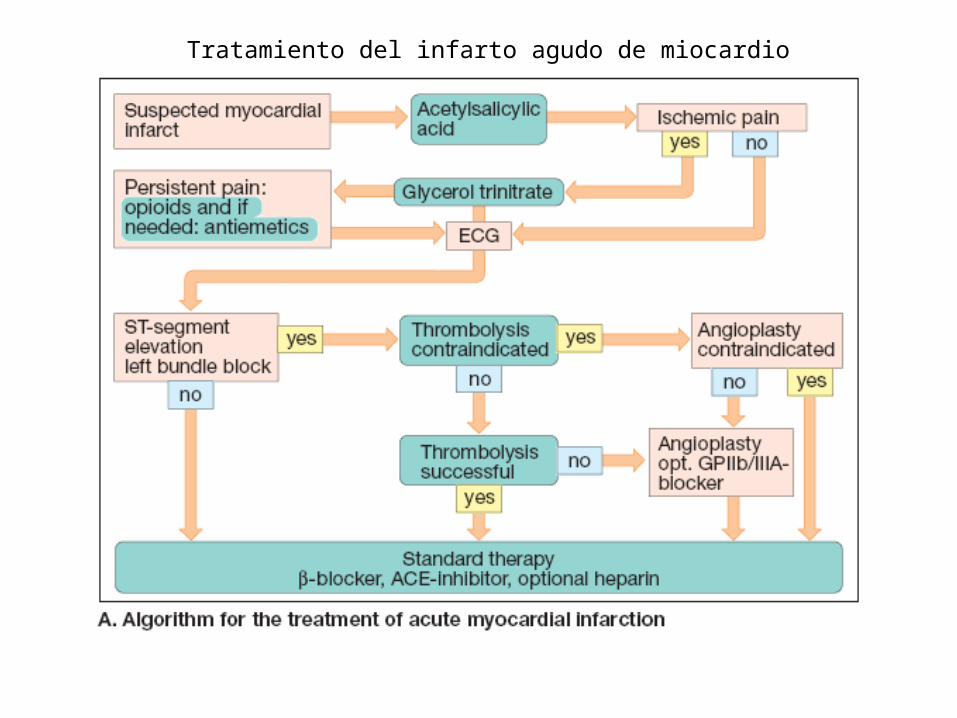
Tratamiento del infarto agudo de miocardio