El virus Zika en Brasil: Relato de una epidemia · Edema MMSS e MMII 51 52,9 116 69,5 0 0 167 N...
34
El virus Zika en Brasil: Relato de una epidemia Carlos Brito
Transcript of El virus Zika en Brasil: Relato de una epidemia · Edema MMSS e MMII 51 52,9 116 69,5 0 0 167 N...

El virus Zika en Brasil:
Relato de una epidemia
Carlos Brito

Dos linajes: Africano y Asiático
Enfermedad nueva, muchas lagunas en la fisiopatogénesis y en las formas clínicas
Pocos estudios publicados en el mundo
Primer brote importante en 2007: Micronesia (Isla de Yap). Población de 11.241
habitantes
Polinesia Francesa 2013: “cambio de comportamiento "
Brote en la Polinesia Francesa en 2013
Cambio de comportamiento con altas tasas de ataque (sintomáticos en la población
en general) y relatos de aparecimiento de complicaciones neurológicas
Población: 268.270 habitantes
Estimativa de casos: 29.000 casos (Tasa de ataque de 10%).
Casos neurológicos sospechosos (Diagnóstico clínico-epidemiológico)
Número de pacientes asintomáticos: 80% (?????)
(Datos anteriores al cambio de estándares y basado en el trabajo I. Yap)
Virus Zika

ZIKA – EPIDEMIA Y COMPLICACIONES NEUROLÓGICAS
Dic
2014
Diciembre
2014
Enero 2015
Brote de
enfermedad
exantemática
diferente del
dengue
Argumentos: RN-PE
Nuevo estándar:
Un brote de
enfermedad
exantemática de
grandes
proporciones.
“Los especialistas
afirman que no es
compatible con el
dengue" = esto de por
sí supone una
investigación.
• Enfermedad de leve
intensidad
• Rash predominante
• Afebril o subfebril
• Artritogénica
• Conjuntivitis
frecuente
Enero-
Feb-
La Epidemia se
propaga por
varios estados del
Nordeste
Alta diseminación
= vector
E. Artritogénica
diferente del
Chikungunya
Zika ? (Kleber
Luz)
Marzo
SSE=PE
Detecta serología
positiva para el
dengue en casos
con el estándar
clínico de la nueva
enfermedad.
Error de
interpretación:
reacción cruzada
28/04
2015 Secretaria de Saúde Secretaria Executiva de Vigilância em Saúde
Avenida Visconde de Suassuna, 658. Santo Amaro – Recife-PE
Fone: (81) 3355-1893- CEP: 50.050-540
observados anteriormente. Quanto ao grupo etário a maior parte dos casos de dengue no grupo
de entrevistados, são adultos jovens (Tabela 3).
Tabela 2. Sinais e sintomas do grupo de casos de dengue entrevistados, confirmados por
laboratório. Recife, janeiro a abril de 2015 Sinais e sintomas Sim Não Ignorado Total
N % N % N % N
Rash 141 84,4 26 15,6 0 0 167
Prurido 141 84,4 26 15,6 0 0 167
Cefaleia 134 89,7 33 19,8 0 0 167
Artralgia 125 75,0 42 25,1 0 0 167
Mialgia 108 66,2 59 35,3 0 0 167
Febre 128 76,6 39 23,4 0 0 167
Dor retro-orbitária 97 61,8 70 41,9 0 0 167
Astenia/Prostação 95 66,2 72 43,1 0 0 167
Edema MMSS e MMII 51 52,9 116 69,5 0 0 167
Náuseas 49 29,4 118 70,7 0 0 167
Dor abdominal 41 30,9 126 75,4 0 0 167
Diarréia 22 11,8 145 86,8 0 0 167
Conjuntivite 32 36,8 135 80,8 0 0 167
Tabela 3. Casos de dengue entrevistados com confirmação laboratorial, por grupo etário. Recife, janeiro a abril de 2015
Grupo Etário
Secretaria de Saúde Secretaria Executiva de Vigilância em Saúde
Avenida Visconde de Suassuna, 658. Santo Amaro – Recife-PE
Fone: (81) 3355-1893- CEP: 50.050-540
NOTA TÉCNICA - 28 de Abril de 2015
Assunto: Situação da Dengue na Cidade do Recife
Em todo o Brasil, assim como na cidade do Recife, os meses de verão são considerados
historicamente como o período vulnerável para a ocorrência de epidemias de dengue em diversas
cidades do país. Ao longo dos anos, epidemias cíclicas têm sido registradas em todo Brasil.
O Recife encontra-se num cenário de epidemia, e até a semana epidemiológica - SE 16,
foram notificados 6.652 casos de dengue e confirmados 2.234 (33,6%). Em 2014, no mesmo
período, foram notificados 728 casos e confirmados 231, representando um aumento de 813,7%
de casos notificados e 867,5% de casos confirmados.
Em Recife não há transmissão ativa do vírus de Chikungunya com comprovação
laboratorial. Para tanto, tem sido mantida a investigação de todos os possíveis casos suspeitos,
com investigação epidemiológica e laboratorial.
Mediante o cenário do crescimento dos casos prováveis de dengue, foram realizadas no
princípio de Janeiro até o mês de Abril, ações de sensibilização para representantes das unidades
de saúde da rede pública municipal e unidades privadas, com o intuito de chamar atenção da
problemática da dengue, além da importância da notificação oficial de todos os casos suspeitos.
Outras medidas de mobilização social foram intensificadas, assim como na Vigilância
Ambiental e Controle de Endemias: as publicações da portaria para implantar ações de controle
nos finais de semana e feriados do mês de março e abril e da portaria para intervenção em
imóveis fechados pelos agentes de saúde ambiental e controle de endemias.
Dentre os diversos sinais e sintomas referidos nas investigações dos casos suspeitos de
dengue, os mais observados em todas as faixas etárias foram: exantema (pequenas manchas
avermelhadas que estão sendo confundidos com uma intoxicação), prurido (coceira), febre ou
febrícula (muitas vezes não referida), mialgia (dores musculares), cefaleia (dor de cabeça),
prostração, dor retro-orbitária (dor nos olhos). Além disso, muitos casos confirmados por
sorologia apresentaram edema de membros superiores e inferiores e em outras partes do corpo.
Zika Virus in Yap State, Micronesia, 2007
positive specimens. The viral RNA concentrations were
≈900–729,000 copies/mL. Most (15 of 17) of the ZIKV-
positive samples were from specimens collected <3 days
after onset; however, 1 specimen (patient 958) collected on
day 11 after onset was positive with an estimated titer of
≈339,000 copies/mL.
Nucleic Acid Sequence and Phylogenetic Analysis
Several RT-PCR–positive serum specimens were se-
lected, and RNA was amplifi ed by RT-PCR to generate
DNA sequence data for the complete coding region. Be-
cause of limited specimen volume, the complete coding
region genome sequence was only obtainable by combin-
ing sequence data from DNA fragments generated from 4
patients. Thus, the designation EC sequence is used to in-
dicate that the sequence was derived from multiple patients
during the epidemic. The exact contribution of sequence
data from each patient is available upon request. However,
the following points should be noted. Approximately 96%
of the complete coding region was obtained from 3 patients;
sequence data from the fourth patient was used primarily to
fi ll in short gaps in the data. Second, ≈50% of the coding re-
gion data was derived from a complete overlap of data from
>2 patients; in these overlap regions the sequence identity
between different patients was ≈100%. Only 2-nt differ-
ences between patients were noted within the overlapping
regions, strongly suggesting that 1 ZIKV strain circulated
during the epidemic.
Percentage identity over the entire coding region of
ZIKV 2007 EC sequence, when compared with the pro-
totype ZIKV (MR 766, isolated in 1947), was 88.9% and
96.5% at the nucleotide and amino acid levels, respectively.
Phylogenetic trees constructed from the complete coding
region of all available fl aviviruses generated by a variety of
methods (neighbor-joining, maximum-parsimony, or min-
imum-evolution) showed the same overall topology, with
the ZIKV prototype and 2007 EC virus placed in a unique
clade (clade 10) within the mosquito-borne fl avivirus clus-
ter previously described by Kuno et al. (16). Alignment
with phylogenetic tree construction by neighbor-joining,
maximum-parsimony, or minimum-evolution algorithms
was also performed for the NS5 region of all available fl a-
viviruses because extensive sequencing and phylogenetic
analysis have been conducted for this region (16).
Three additional ZIKV strains isolated from Senegal
in 1984 and sequenced in this study were also included in
a tree. This NS5 tree demonstrated similar topology to the
complete coding region tree, with all ZIKVs placed within
a unique clade (clade 10) along with SPOV. Figure 1 shows
the NS5 tree with only mosquito-borne fl aviviruses (clus-
ter) displayed. This NS5 tree also shows that within the
Zika/Spondweni clade there appear to be 3 branches among
ZIKVs: Nigerian ZIKVs, prototype MR766, and 2007 Yap
virus. Percentage identity among these ZIKVs confi rms
the tree topology, in which ZIKV 2007 EC is most distally
related to East and West African ZIKV strains (data not
shown).
The predicted amino acid sequence of ZIKV 2007 EC
contains the Asn-X-Ser/Thr glycosylation motif at posi-
tion 154 in the envelope glycoprotein, found in many fl a-
viviruses, yet absent by deletion in the prototype ZIKV
MR 766. This region of the prototype virus, along with
3 ZIKVs isolated from Senegal in 1984, was sequenced
(Figure 2). Included in this alignment is a ZIKV isolate
from GenBank (accession no. AF372422). Sequencing
confi rmed that prototype ZIKV MR766 has a 4-aa (12-nt)
deletion when compared with ZIKV 2007 EC virus and
ZIKVs from Senegal.
Discussion
Historically, ZIKV has rarely been associated with hu-
man disease, with only 1 small cluster of human cases in
Indonesia reported (9). We report a widespread epidemic
of human disease associated with ZIKV in Yap State in
2007. ZIKV epidemics may have occurred but been mis-
diagnosed as dengue because of similar clinical symptoms
and serologic cross-reactivity with DENVs. Our serologic
data indicate that ZIKV-infected patients can be positive
in an IgM assay for DENVs, particularly if ZIKV is a sec-
ondary fl avivirus infection. If ZIKV is the fi rst fl avivirus
encountered, our data indicate that cross-reactivity is mini-
mal. However, when ZIKV infection occurs after a fl avi-
virus infection, our data indicate that the extent of cross-
reactivity in the IgM assay is greater. Therefore, if ZIKV
infections occur in a population with DENV (or other fl a-
vivirus) background immunity, our data suggest that exten-
sive cross-reactivity in the dengue IgM assay will occur,
which could lead to the erroneous conclusion that dengue
caused the epidemic. Whether this cross-reactivity has oc-
curred is open to speculation. However, reexamination of
specimens from dengue epidemics may provide an answer.
In addition, use of virus isolation or RT-PCR for labora-
tory diagnosis of dengue infections would also prevent this
misinterpretation. Therefore, use of virus detection assays
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 14, No. 8, August 2008 1237
Figure 2. Alignment of nucleotide and amino acid sequences
adjacent to the envelope (ENV)–154 glycosylation site of Zika virus
strains. Dashes indicate deletions. EC, epidemic consensus.
1321
Zika MR766 1947 Uganda ATGATTGGA------------TATGAAACTGACGAAGATAGAGCG
Zika AF372422 ATGATTGTTAATGAT------------------GAAAACAGAGCA
Zika 41662 Senegal 1984 ATGATTGTGAATGACACAGGACATGAAACTGACGAAAACAGAGCA
Zika 41524 Senegal 1984 ATGATTGTGAATGACACAGGACATGAAACTGACGAAAACAGAGCA
Zika 41525 Senegal 1984 ATGATTGTGAATGACACAGGACATGAAACTGACGAAAACAGAGCA
Zika 2007 EC Yap ATGATCGTTAATGACACAGGACATGAAACTGATGAGAATAGAGCG
ENV-151 ENV-164
Zika MR766 1947 Uganda MetIleGly------------TyrGluThrAspGluAspArgAla
Zika AF372422 MetIleValAsnAsp------------------GluAsnArgAla
Zika 41662 Senegal 1984 MetIleValAsnAspThrGlyHisGluThrAspGluAsnArgAla
Zika 41524 Senegal 1984 MetIleValAsnAspThrGlyHisGluThrAspGluAsnArgAla
Zika 41525 Senegal 1984 MetIleValAsnAspThrGlyHisGluThrAspGluAsnArgAla
Zika 2007 EC Yap MetIleValAsnAspThrGlyHisGluThrAspGluAsnArgAla
Zika virus (ZIKV) is a mosquito-borne fl avivirus fi rst
isolated in Uganda from a sentinel monkey in 1947. Mos-
quito and sentinel animal surveillance studies have dem-
onstrated that ZIKV is endemic to Africa and Southeast
Asia, yet reported human cases are rare with <10 cases
reported in the literature. In June 2007, an epidemic of fe-
ver and rash associated with ZIKV was detected in Yap
State, Federated States of Micronesia. We report the ge-
netic and serologic properties of the ZIKV associated with
this epidemic.
Zika virus (ZIKV) is a mosquito-transmitted virus in the
family Flaviviridae and genus Flavivirus. It was ini-
tially isolated in 1947 from blood of a febrile sentinel rhe-
sus monkey during a yellow fever study in the Zika forest
of Uganda (1). The virus was subsequently isolated from
a pool of Aedes africanus mosquitoes collected in 1948
from the same region of the Zika forest; a serologic survey
conducted at that time showed that 6.1% of the residents
in nearby regions of Uganda had specifi c antibodies to
ZIKV (1,2).
Over the next 20 years, several ZIKV isolates were
obtained from Aedes spp. in Africa (Ae. africanus) and
Malaysia (Ae. aegypti), implicating these species as likely
epidemic or enzootic vectors (3–5). Several ZIKV human
isolates were also obtained in the 1960s and 1970s from
East and West Africa during routine arbovirus surveillance
studies in the absence of epidemics (6–8). Additional se-
rologic studies in the 1950s and 1960s detected ZIKV in-
fections among humans in Egypt, Nigeria, Uganda, India,
Malaysia, Indonesia, Pakistan, Thailand, North Vietnam,
and the Philippines (5). These data strongly suggest wide-
spread occurrence of ZIKV from Africa to Southeast Asia
west and north of the Wallace line.
In 1977, ZIKV infection was confi rmed among 7 pa-
tients in central Java, Indonesia, during an acute fever study
(9). Data on these 7 ZIKV cases and several previously re-
ported human infections indicated that clinical characteris-
tics of infection with ZIKV included fever, headache, mal-
aise, stomach ache, dizziness, anorexia, and maculopapular
rash; in all cases infection appeared relatively mild, self-
limiting, and nonlethal (6,8–10).
In April 2007, an epidemic of rash, conjunctivitis, and
arthralgia was noted by physicians in Yap State, Federated
States of Micronesia (11). Laboratory testing with a rapid
assay suggested that a dengue virus (DENV) was the caus-
ative agent. In June 2007, samples were sent for confi rma-
tory testing to the Arbovirus Diagnostic Laboratory at the
Centers for Disease Control and Prevention (CDC, Fort
Collins, CO, USA). Serologic testing by immunoglobu-
lin (Ig) M–capture ELISA with DENV antigen confi rmed
recent fl avivirus infection in several patients. Testing by
reverse transcription–PCR (RT-PCR) with fl avivirus con-
sensus primers generated DNA fragments, which when
subjected to nucleic acid sequencing, demonstrated ≈90%
nucleotide identity with ZIKV. These fi ndings indicated
that ZIKV was the causative agent of the Yap epidemic.
We report serologic parameters of the immune response
Genetic and Serologic Properties
of Zika Virus Associated with
an Epidemic, Yap State,
Micronesia, 2007
Robert S. Lanciotti,* Olga L. Kosoy,* Janeen J. Laven,* Jason O. Velez,* Amy J. Lambert,*
Alison J. Johnson,* Stephanie M. Stanfi eld,* and Mark R. Duffy*
RESEARCH
1232 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 14, No. 8, August 2008
*Centers for Disease Control and Prevention, Fort Collins, Colo-
rado, USA
DOI: 10.3201/eid1408.080287

Se confirma la hipótesis de epidemia por Zika en Brasil en abril de 2015
PCR realizado en 8 de un total de 25 muestras de sangre de casos sospechosos de
Bahia (Universidad Federal de Bahia) y
Posteriormente, en 8 de un total de 21 casos de Rio Grande do Norte (Fiocruz/PR).
Virus Zika
database used would require optimization with addition of
reference spectra for the organism and its close relatives
(e.g., B. thailandensis). B. pseudomallei, although differ-
ent from other Burkholderia spp. in its pathogenicity and
epidemiology, is not easily discriminated from B. thailand-
ensis or B. cepacia complex by using phenotypic tests (10).
In summary, infection with B. pseudomallei should be
considered in patients with pneumonia after travel to the
Baja Peninsula in Mexico, and especially after an extreme
weather event. Because of risk for transmission to laborato-
ry workers and the potential for B. pseudomallei to be used
for bioterrorism, clinical laboratories should perform only
limited work up of suspected isolates before referring them
to a public health laboratory for defin
i
tive ident ifica
t
i on.
Acknowledgment
We used the Multi-Locus Sequence Typing website
(http://www.mlst.net) at Imperial College London, developed by
David Aanensen and supported by the Wellcome Trust.
References 1. Currie BJ, Dance DA, Cheng AC. The global distribution of
Burkholderia pseudomallei and meliodosis: an update. Trans R Soc
Trop Med Hyg. 2008;102(Suppl 1):S1–4. http://dx.doi.org/10.1016/
S0035-9203(08)70002-6
2. Inglis TJ, Rolim DB, Sousa AQ. Melioidosis in the Americas.
Am J Trop Med Hyg. 2006;75:947–54.
3. Centers for Disease Control and Prevention. Melioidosis: risk of
exposure, January 26, 2012 [cited 2014 Dec 19]. http://www.cdc.gov/
melioidosis/exposure/index.html
4. Currie BJ. Melioidosis: evolving concepts in epidemiology,
pathogenesis, and treatment. Semin Respir Crit Care Med.
2015;36:111–25. http://dx.doi.org/10.1055/s-0034-1398389
5. Schweizer HP, Limmathurotsakul D, Peacock SJ. New insights
from the 7th World Melioidosis Congress 2013. Emerg Infect Dis.
2014;20:e131737.
6. Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med.
2012;367:1035–44. http://dx.doi.org/10.1056/NEJMra1204699
7. Gee JE, Allender CJ, Tuanvok A, Elrod MG, Hoffmaster AR.
Burkholderia pseudomallei type G in Western Hemisphere.
Emerg Infect Dis. 2014;20:682–4. http://dx.doi.org/10.3201/
eid2004.130960
8. Pitman MC, Luck T, Marshall CS, Anstey NM, Ward L, Currie BJ.
Intravenous therapy duration and outcomes in melioidosis: a new
treatment paradigm. PLoS Negl Trop Dis. 2015;9:e0003586.
http://dx.doi.org/10.1371/journal.pntd.0003586
9. Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD,
Cheng AC, et al. Workshop on treatment of and postexposure
prophylaxis for Burkholderia pseudomallei and B. mallei infection,
2010. Emerg Infect Dis. 2012;18:e2. http://dx.doi.org/10.3201/
eid1812.120638
10. Zong Z, Wang X, Deng Y, Zhou T. Misidentific
a
t ion of
Burkholderia pseudomallei as Burkholderia cepacia by the
Vitek 2 system. J Med Microbiol. 2012;61:1483–4.
http://dx.doi.org/10.1099/jmm.0.041525-0
Address for correspondence: Jennifer W. Cheng, Department of
Infectious Disease, Rush University Medical Center, 600 S Paulina St,
Ste 143, Chicago, IL 60612, USA; email: [email protected]
Zika Virus Outbreak, Bahia, Brazil
Gubio S. Campos, Antonio C. Bandeira,
Silvia I. Sardi
Authors affil
i
at ions: Feder al Un i ver si ty of Bahi a, Sal vador ,
Bahia, Brazil (G.S. Campos, S.I. Sardi); Hospital Aliança, Salvador
(A.C. Bandeira)
DOI: http://dx.doi.org/10.32301/eid2110.150847
To the Editor: Zika virus (ZIKV) is a mosquito-
borne flav i vi rus related to yellow fever virus, dengue virus
(DENV), and West Nile virus (WNV). It is a single-strand-
ed positive RNA virus (10,794-nt genome) that is closely
related to the Spondweni virus and is transmitted by many
Aedes spp. mosquitoes, including Ae. africanus, Ae. lu-
teocephalus, Ae. hensilli, and Ae. aegypti. The virus was
identifie
d
in rhesus monkeys during sylvatic yellow fever
surveillance in the Zika Forest in Uganda in 1947 and was
reported in humans in 1952 (1).
In 2007, an outbreak of ZIKV was reported in Yap Is-
land, Federated States of Micronesia (2). ZIKV also caused
a major epidemic in the French Polynesia in 2013–2014 (3),
and New Caledonia reported imported cases from French
Polynesia in 2013 and reported an outbreak in 2014 (4).
A new challenge has arisen in Brazil with the emer-
gence of ZIKV and co-circulation with others arboviruses
(i.e., DENV and chikungunya virus [CHIKV]). We report
ZIKV infection in Brazil associated with a recent ongoing
outbreak in Camaçari, Bahia, Brazil, of an illness charac-
terized by maculopapular rash, fever, myalgias/arthralgia,
and conjunctivitis.
On March 26, 2015, serum samples were obtained
from 24 patients (Table) at Santa Helena Hospital in Cama-
çari who were given a presumptive diagnosis of an acute
viral illness by emergency department physicians. These
patients were given treatment for a dengue-like illness, and
blood samples were obtained for complete blood counts
and serologic testing by using an ELISA specific for IgG
and IgM against DENV.
Serum samples were analyzed at the Federal Univer-
sity of Bahia by reverse transcription PCR (RT-PCR) to
detect DENV, CHIKV, WNV, Mayaro virus, and ZIKV.
In brief, serum samples were subjected to RNA extrac-
tion by using the QIAamp Viral RNA Mini Kit (QIAGEN,
Hilden, Germany). RNA was reverse transcribed by using
the SuperScript II Reverse Transcription Kit (Invitrogen,
Carlsbad, CA, USA) and subjected to PCRs specific for
DENV (5) CHIKV (6), WNV (7) and Mayaro virus (8).
A positive RT-PCR for a partial region of the envelope
gene with primers ZIKVENF and ZIKVENVR (positions
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 10, October 2015 1885
LETTERS
database used would require optimization with addition of
reference spectra for the organism and its close relatives
(e.g., B. thailandensis). B. pseudomallei, although differ-
ent from other Burkholderia spp. in its pathogenicity and
epidemiology, is not easily discriminated from B. thailand-
ensis or B. cepacia complex by using phenotypic tests (10).
In summary, infection with B. pseudomallei should be
considered in patients with pneumonia after travel to the
Baja Peninsula in Mexico, and especially after an extreme
weather event. Because of risk for transmission to laborato-
ry workers and the potential for B. pseudomallei to be used
for bioterrorism, clinical laboratories should perform only
limited work up of suspected isolates before referring them
to a public health laboratory for defin
i
tive ident ifica
t
i on.
Acknowledgment
We used the Multi-Locus Sequence Typing website
(http://www.mlst.net) at Imperial College London, developed by
David Aanensen and supported by the Wellcome Trust.
References 1. Currie BJ, Dance DA, Cheng AC. The global distribution of
Burkholderia pseudomallei and meliodosis: an update. Trans R Soc
Trop Med Hyg. 2008;102(Suppl 1):S1–4. http://dx.doi.org/10.1016/
S0035-9203(08)70002-6
2. Inglis TJ, Rolim DB, Sousa AQ. Melioidosis in the Americas.
Am J Trop Med Hyg. 2006;75:947–54.
3. Centers for Disease Control and Prevention. Melioidosis: risk of
exposure, January 26, 2012 [cited 2014 Dec 19]. http://www.cdc.gov/
melioidosis/exposure/index.html
4. Currie BJ. Melioidosis: evolving concepts in epidemiology,
pathogenesis, and treatment. Semin Respir Crit Care Med.
2015;36:111–25. http://dx.doi.org/10.1055/s-0034-1398389
5. Schweizer HP, Limmathurotsakul D, Peacock SJ. New insights
from the 7th World Melioidosis Congress 2013. Emerg Infect Dis.
2014;20:e131737.
6. Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med.
2012;367:1035–44. http://dx.doi.org/10.1056/NEJMra1204699
7. Gee JE, Allender CJ, Tuanvok A, Elrod MG, Hoffmaster AR.
Burkholderia pseudomallei type G in Western Hemisphere.
Emerg Infect Dis. 2014;20:682–4. http://dx.doi.org/10.3201/
eid2004.130960
8. Pitman MC, Luck T, Marshall CS, Anstey NM, Ward L, Currie BJ.
Intravenous therapy duration and outcomes in melioidosis: a new
treatment paradigm. PLoS Negl Trop Dis. 2015;9:e0003586.
http://dx.doi.org/10.1371/journal.pntd.0003586
9. Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD,
Cheng AC, et al. Workshop on treatment of and postexposure
prophylaxis for Burkholderia pseudomallei and B. mallei infection,
2010. Emerg Infect Dis. 2012;18:e2. http://dx.doi.org/10.3201/
eid1812.120638
10. Zong Z, Wang X, Deng Y, Zhou T. Misidentific
a
t ion of
Burkholderia pseudomallei as Burkholderia cepacia by the
Vitek 2 system. J Med Microbiol. 2012;61:1483–4.
http://dx.doi.org/10.1099/jmm.0.041525-0
Address for correspondence: Jennifer W. Cheng, Department of
Infectious Disease, Rush University Medical Center, 600 S Paulina St,
Ste 143, Chicago, IL 60612, USA; email: [email protected]
Zika Virus Outbreak, Bahia, Brazil
Gubio S. Campos, Antonio C. Bandeira,
Silvia I. Sardi
Authors affil
i
at ions: Feder al Un i ver si ty of Bahi a, Sal vador ,
Bahia, Brazil (G.S. Campos, S.I. Sardi); Hospital Aliança, Salvador
(A.C. Bandeira)
DOI: http://dx.doi.org/10.32301/eid2110.150847
To the Editor: Zika virus (ZIKV) is a mosquito-
borne flav i vi rus related to yellow fever virus, dengue virus
(DENV), and West Nile virus (WNV). It is a single-strand-
ed positive RNA virus (10,794-nt genome) that is closely
related to the Spondweni virus and is transmitted by many
Aedes spp. mosquitoes, including Ae. africanus, Ae. lu-
teocephalus, Ae. hensilli, and Ae. aegypti. The virus was
identifie
d
in rhesus monkeys during sylvatic yellow fever
surveillance in the Zika Forest in Uganda in 1947 and was
reported in humans in 1952 (1).
In 2007, an outbreak of ZIKV was reported in Yap Is-
land, Federated States of Micronesia (2). ZIKV also caused
a major epidemic in the French Polynesia in 2013–2014 (3),
and New Caledonia reported imported cases from French
Polynesia in 2013 and reported an outbreak in 2014 (4).
A new challenge has arisen in Brazil with the emer-
gence of ZIKV and co-circulation with others arboviruses
(i.e., DENV and chikungunya virus [CHIKV]). We report
ZIKV infection in Brazil associated with a recent ongoing
outbreak in Camaçari, Bahia, Brazil, of an illness charac-
terized by maculopapular rash, fever, myalgias/arthralgia,
and conjunctivitis.
On March 26, 2015, serum samples were obtained
from 24 patients (Table) at Santa Helena Hospital in Cama-
çari who were given a presumptive diagnosis of an acute
viral illness by emergency department physicians. These
patients were given treatment for a dengue-like illness, and
blood samples were obtained for complete blood counts
and serologic testing by using an ELISA specific for IgG
and IgM against DENV.
Serum samples were analyzed at the Federal Univer-
sity of Bahia by reverse transcription PCR (RT-PCR) to
detect DENV, CHIKV, WNV, Mayaro virus, and ZIKV.
In brief, serum samples were subjected to RNA extrac-
tion by using the QIAamp Viral RNA Mini Kit (QIAGEN,
Hilden, Germany). RNA was reverse transcribed by using
the SuperScript II Reverse Transcription Kit (Invitrogen,
Carlsbad, CA, USA) and subjected to PCRs specific for
DENV (5) CHIKV (6), WNV (7) and Mayaro virus (8).
A positive RT-PCR for a partial region of the envelope
gene with primers ZIKVENF and ZIKVENVR (positions
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 10, October 2015 1885
LETTERS

Caso sospechoso:
Aquellos que presentan evidencias clínicas y epidemiológicas (con antecedentes recientes, proceden del área con casos confirmados, endémicos o epidémicos). Ej: Dengue, Zika, Chikungunya.
Caso confirmado por laboratorio:
Cualquier caso sospechoso confirmado por exámenes específicos.
Caso confirmado por Criterio clínico-epidemiológico:
Durante el brote de los primeros casos, todos los esfuerzos deben concentrarse para asegurar el diagnóstico laboratorial. Sin embargo, una vez declarada la transmisión, no todos los pacientes necesitarán la confirmación laboratorial.
El caso podrá ser notificado (confirmado), como el de la infección sospechosa, con base en criterios clínicos-epidemiológicos.
Reservar las pruebas de laboratorio, en este contexto, para los casos graves o con cuadros atípicos.
DEFINICIÓN DE CASOS - NOTIFICACIÓN
Carlos Brito UFPE

Definición: Pacientes que presenten:
Ausencia de fiebre o fiebre, medida o referida, hasta 38,5°C E, exantema máculopapular pruriginoso que aparece dentro de las 72 horas posteriores a los primeiros síntomas, acompañado de por lo menos UNO de los siguientes signos y síntomas:
Hiperemia conjuntival no purulenta (ojos rojos) O
Artralgia O
Edema en miembros
con antecedente epidemiológico positivo
Diferencial: Dengue, Chikungunya, Sarampión y Rubeola principalmente.
Definición del caso Zika:
Exantema máculopapular pruriginoso que ocurre 72 horas despúes de los primeros síntomas, sin fiebre o fiebre referida o fiebre medida ≤ 38,5 C E, pudiendo presentar los siguientes signos y síntomas:
Hiperemia conjuntival (no purulenta)
Artralgia
Edema articular
DEFINICIÓN DE CASOS - ZIKA

• Estudio de base hospitalaria, descriptivo, serie de casos
Periodo de estudio
De enero a julio de 2015
Fuente de datos
• Historia clínica de la emergencia
Lugar de estudio
Hospital Santa Joana (Privado-Referencia en la atención
de emergencias del polo médico de Recife)
Investigación Dengue-Zika – Unidad de Emergencia
Carlos Brito UFPE

Resultados preliminares
Historias clínicas analizadas 335 (T: 900) Total: 900
Excluidos 1 1
Inconcluyente, faltan
datos/síntomas
49 Faltan datos (No figura el tiempo de
enfermedad o de rash)
Duplicidad 30 Más de una atención
N=802
Diagnóstico Zika Dengue Inconcluyente Otros N 585 101 25 11
% 81% 14% 3% 2%
Pérdidas: 6,23%
73
164
303
182
Jan Fev Março Abril
N casos/mes

Variable n (%)
Sexo femenino 354 (60,5)
Mediana (Intervalo)
Edad (años) 31 (5m - 79)
Rango de edad n (%)
0 – 14 años 149 (25,5)
15 – 49 años 344 (58,8)
> 50 años 92 (15,7)
Casos Zika N=585
Rango de edad N %
0-4 71 12,1
5-9 A 42 7,2
10-14 A 36 6,2
15-19 A 38 6,5
20-39 A 237 40,5
40-59 125 21,4
>60 A 36 6,2
Total 585 100,0
Carlos Brito UFPE

Variable Mediana (Intervalo)
Fecha IS - 1ª Atención (días) 2 (8h – 7)
Fiebre en la 1ª atención n (%)
Fiebre referida/medida 73 (30)
Fiebre>38,5 2 (2,7)
N=244
Resultados preliminares
292
173 179 166
143
72
29 16 15 13 10 12
0
50
100
150
200
250
300
350 Síntoma 585
Prurito 49,9
Cefalea 29,6
Mialgia 30,6
Astenia 28,4
Artralgia 24,4
Dolor retro-orbitario 12,3
Edema articulaciones 5,0
Adenomegalia 2,7
Conjuntivitis 2,6
Dolor de garganta 2,2
Diarrea 1,7
Vómitos 2,1

DIAGNÓSTICO DIFERENCIAL DE DENGUE, ZIKA Y CHIKUNGUNYA
Exantema Aparece a partir del
cuarto día Aparece en el primer o
segundo día Aparece 2-5 día
30-50% de los casos 90-100% de los casos
Frecuencia 50% de los casos
Aspectos Clínico/Laboratorial
Dengue Zika Chikungunya
Fiebre/estándares Más de 38°C Sin fiebre o subfebril
(≤ 38,5°C) Fiebre alta > 38°C
Alta (Varias x/día) Fiebre leve (1-2x/día) Alta en 1-2 día
Duración 4 a 7 días 1-2 días 2-3 días
Mialgia (Frecuencia)
+++ ++ +
Artralgia (frecuencia)
+ ++ +++
Intensidad del dolor articular
Leve Leve/Moderado Moderado/Severo
Edema articulaciones Raro Frecuente, leve intensidad Frecuente, moderado a severo Conjuntivitis Raro 50-90% de los casos 30%
Cefalea +++ ++ ++
Hipertrofia ganglionar + +++ ++
Discrasia sanguínea ++ ausente +
Riesgo de muerte Existe (+++) Existe (?)* Existe (+)
Complicación Neurológica ++ +++ (?) + (predominante en Neonatos)
Leucopenia +++ +++ +++
Linfopenia Infrecuente Infrecuente Frecuente
Trombocitopenia +++ Ausente +

ZIKA – EPIDEMIA Y COMPLICACIONES NEUROLÓGICAS
Dic
2014
Diciembre
2014/
Enero 2015
Brote
enfermedad
exantemática
diferente del
dengue
Argumentos: RN-PE
Nuevos estándares:
Un brote de E.
exantemática de
grandes
proporciones.
“Los especialistas
afirman que no es
compatible con el
dengue" = esto de por
sí supone una
investigación.
• Enfermedad de leve
intensidad
• Rash predominante
• Afebril o subfebril
• Artritogénica
• Conjuntivitis
frecuente
Enero-
Feb-
Aumento de casos
neurológicos (RN,
PE, BA)
Pernambuco
Emitimos un alerta a los
neurólogos, via
whatsApp, sobre el
riesgo de aumento de
los casos neurológicos
Dr. Iris Machado / Dra.
Lucia Brito - HR
(contestan
positivamente)
15 mayo
2015
En visita al HR:
Gran número de
casos, superior a
los años
anteriores.
Entrevisto a los
pacientes: “Cuadro
clinico viral,
antecedente de
Zika"
Hipótesis de la
Polinesia Francesa
se confirma
FIOCRUZ-PE
(LAVITE)
Confirma 7 casos
neurológicos por
PCR y aislamiento
viral Zika +
Junio
2015
Nuevo
aumento de
los casos
neurológicos
en diciembre
de 2015
Nov/Dic
2015
Número de casos
con aumento
progresivo
Mayo/junio
2015
La epidemia se
propaga por
varios estados del
Nordeste
Alta diseminación
= vector
E. Artritogénica
diferente del
Chikungunya
Zika ? (Kleber
Luz)
Marzo
database used would require optimization with addition of
reference spectra for the organism and its close relatives
(e.g., B. thailandensis). B. pseudomallei, although differ-
ent from other Burkholderia spp. in its pathogenicity and
epidemiology, is not easily discriminated from B. thailand-
ensis or B. cepacia complex by using phenotypic tests (10).
In summary, infection with B. pseudomallei should be
considered in patients with pneumonia after travel to the
Baja Peninsula in Mexico, and especially after an extreme
weather event. Because of risk for transmission to laborato-
ry workers and the potential for B. pseudomallei to be used
for bioterrorism, clinical laboratories should perform only
limited work up of suspected isolates before referring them
to a public health laboratory for defin
i
tive ident ifica
t
i on.
Acknowledgment
We used the Multi-Locus Sequence Typing website
(http://www.mlst.net) at Imperial College London, developed by
David Aanensen and supported by the Wellcome Trust.
References 1. Currie BJ, Dance DA, Cheng AC. The global distribution of
Burkholderia pseudomallei and meliodosis: an update. Trans R Soc
Trop Med Hyg. 2008;102(Suppl 1):S1–4. http://dx.doi.org/10.1016/
S0035-9203(08)70002-6
2. Inglis TJ, Rolim DB, Sousa AQ. Melioidosis in the Americas.
Am J Trop Med Hyg. 2006;75:947–54.
3. Centers for Disease Control and Prevention. Melioidosis: risk of
exposure, January 26, 2012 [cited 2014 Dec 19]. http://www.cdc.gov/
melioidosis/exposure/index.html
4. Currie BJ. Melioidosis: evolving concepts in epidemiology,
pathogenesis, and treatment. Semin Respir Crit Care Med.
2015;36:111–25. http://dx.doi.org/10.1055/s-0034-1398389
5. Schweizer HP, Limmathurotsakul D, Peacock SJ. New insights
from the 7th World Melioidosis Congress 2013. Emerg Infect Dis.
2014;20:e131737.
6. Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med.
2012;367:1035–44. http://dx.doi.org/10.1056/NEJMra1204699
7. Gee JE, Allender CJ, Tuanvok A, Elrod MG, Hoffmaster AR.
Burkholderia pseudomallei type G in Western Hemisphere.
Emerg Infect Dis. 2014;20:682–4. http://dx.doi.org/10.3201/
eid2004.130960
8. Pitman MC, Luck T, Marshall CS, Anstey NM, Ward L, Currie BJ.
Intravenous therapy duration and outcomes in melioidosis: a new
treatment paradigm. PLoS Negl Trop Dis. 2015;9:e0003586.
http://dx.doi.org/10.1371/journal.pntd.0003586
9. Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD,
Cheng AC, et al. Workshop on treatment of and postexposure
prophylaxis for Burkholderia pseudomallei and B. mallei infection,
2010. Emerg Infect Dis. 2012;18:e2. http://dx.doi.org/10.3201/
eid1812.120638
10. Zong Z, Wang X, Deng Y, Zhou T. Misidentific
a
t ion of
Burkholderia pseudomallei as Burkholderia cepacia by the
Vitek 2 system. J Med Microbiol. 2012;61:1483–4.
http://dx.doi.org/10.1099/jmm.0.041525-0
Address for correspondence: Jennifer W. Cheng, Department of
Infectious Disease, Rush University Medical Center, 600 S Paulina St,
Ste 143, Chicago, IL 60612, USA; email: [email protected]
Zika Virus Outbreak, Bahia, Brazil
Gubio S. Campos, Antonio C. Bandeira,
Silvia I. Sardi
Authors affil
i
at ions: Feder al Un i ver si ty of Bahi a, Sal vador ,
Bahia, Brazil (G.S. Campos, S.I. Sardi); Hospital Aliança, Salvador
(A.C. Bandeira)
DOI: http://dx.doi.org/10.32301/eid2110.150847
To the Editor: Zika virus (ZIKV) is a mosquito-
borne flav i vi rus related to yellow fever virus, dengue virus
(DENV), and West Nile virus (WNV). It is a single-strand-
ed positive RNA virus (10,794-nt genome) that is closely
related to the Spondweni virus and is transmitted by many
Aedes spp. mosquitoes, including Ae. africanus, Ae. lu-
teocephalus, Ae. hensilli, and Ae. aegypti. The virus was
identifie
d
in rhesus monkeys during sylvatic yellow fever
surveillance in the Zika Forest in Uganda in 1947 and was
reported in humans in 1952 (1).
In 2007, an outbreak of ZIKV was reported in Yap Is-
land, Federated States of Micronesia (2). ZIKV also caused
a major epidemic in the French Polynesia in 2013–2014 (3),
and New Caledonia reported imported cases from French
Polynesia in 2013 and reported an outbreak in 2014 (4).
A new challenge has arisen in Brazil with the emer-
gence of ZIKV and co-circulation with others arboviruses
(i.e., DENV and chikungunya virus [CHIKV]). We report
ZIKV infection in Brazil associated with a recent ongoing
outbreak in Camaçari, Bahia, Brazil, of an illness charac-
terized by maculopapular rash, fever, myalgias/arthralgia,
and conjunctivitis.
On March 26, 2015, serum samples were obtained
from 24 patients (Table) at Santa Helena Hospital in Cama-
çari who were given a presumptive diagnosis of an acute
viral illness by emergency department physicians. These
patients were given treatment for a dengue-like illness, and
blood samples were obtained for complete blood counts
and serologic testing by using an ELISA specific for IgG
and IgM against DENV.
Serum samples were analyzed at the Federal Univer-
sity of Bahia by reverse transcription PCR (RT-PCR) to
detect DENV, CHIKV, WNV, Mayaro virus, and ZIKV.
In brief, serum samples were subjected to RNA extrac-
tion by using the QIAamp Viral RNA Mini Kit (QIAGEN,
Hilden, Germany). RNA was reverse transcribed by using
the SuperScript II Reverse Transcription Kit (Invitrogen,
Carlsbad, CA, USA) and subjected to PCRs specific for
DENV (5) CHIKV (6), WNV (7) and Mayaro virus (8).
A positive RT-PCR for a partial region of the envelope
gene with primers ZIKVENF and ZIKVENVR (positions
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 10, October 2015 1885
LETTERS
database used would require optimization with addition of
reference spectra for the organism and its close relatives
(e.g., B. thailandensis). B. pseudomallei, although differ-
ent from other Burkholderia spp. in its pathogenicity and
epidemiology, is not easily discriminated from B. thailand-
ensis or B. cepacia complex by using phenotypic tests (10).
In summary, infection with B. pseudomallei should be
considered in patients with pneumonia after travel to the
Baja Peninsula in Mexico, and especially after an extreme
weather event. Because of risk for transmission to laborato-
ry workers and the potential for B. pseudomallei to be used
for bioterrorism, clinical laboratories should perform only
limited work up of suspected isolates before referring them
to a public health laboratory for defin
i
tive ident ifica
t
i on.
Acknowledgment
We used the Multi-Locus Sequence Typing website
(http://www.mlst.net) at Imperial College London, developed by
David Aanensen and supported by the Wellcome Trust.
References 1. Currie BJ, Dance DA, Cheng AC. The global distribution of
Burkholderia pseudomallei and meliodosis: an update. Trans R Soc
Trop Med Hyg. 2008;102(Suppl 1):S1–4. http://dx.doi.org/10.1016/
S0035-9203(08)70002-6
2. Inglis TJ, Rolim DB, Sousa AQ. Melioidosis in the Americas.
Am J Trop Med Hyg. 2006;75:947–54.
3. Centers for Disease Control and Prevention. Melioidosis: risk of
exposure, January 26, 2012 [cited 2014 Dec 19]. http://www.cdc.gov/
melioidosis/exposure/index.html
4. Currie BJ. Melioidosis: evolving concepts in epidemiology,
pathogenesis, and treatment. Semin Respir Crit Care Med.
2015;36:111–25. http://dx.doi.org/10.1055/s-0034-1398389
5. Schweizer HP, Limmathurotsakul D, Peacock SJ. New insights
from the 7th World Melioidosis Congress 2013. Emerg Infect Dis.
2014;20:e131737.
6. Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med.
2012;367:1035–44. http://dx.doi.org/10.1056/NEJMra1204699
7. Gee JE, Allender CJ, Tuanvok A, Elrod MG, Hoffmaster AR.
Burkholderia pseudomallei type G in Western Hemisphere.
Emerg Infect Dis. 2014;20:682–4. http://dx.doi.org/10.3201/
eid2004.130960
8. Pitman MC, Luck T, Marshall CS, Anstey NM, Ward L, Currie BJ.
Intravenous therapy duration and outcomes in melioidosis: a new
treatment paradigm. PLoS Negl Trop Dis. 2015;9:e0003586.
http://dx.doi.org/10.1371/journal.pntd.0003586
9. Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD,
Cheng AC, et al. Workshop on treatment of and postexposure
prophylaxis for Burkholderia pseudomallei and B. mallei infection,
2010. Emerg Infect Dis. 2012;18:e2. http://dx.doi.org/10.3201/
eid1812.120638
10. Zong Z, Wang X, Deng Y, Zhou T. Misidentific
a
t ion of
Burkholderia pseudomallei as Burkholderia cepacia by the
Vitek 2 system. J Med Microbiol. 2012;61:1483–4.
http://dx.doi.org/10.1099/jmm.0.041525-0
Address for correspondence: Jennifer W. Cheng, Department of
Infectious Disease, Rush University Medical Center, 600 S Paulina St,
Ste 143, Chicago, IL 60612, USA; email: [email protected]
Zika Virus Outbreak, Bahia, Brazil
Gubio S. Campos, Antonio C. Bandeira,
Silvia I. Sardi
Authors affil
i
at ions: Feder al Un i ver si ty of Bahi a, Sal vador ,
Bahia, Brazil (G.S. Campos, S.I. Sardi); Hospital Aliança, Salvador
(A.C. Bandeira)
DOI: http://dx.doi.org/10.32301/eid2110.150847
To the Editor: Zika virus (ZIKV) is a mosquito-
borne flav i vi rus related to yellow fever virus, dengue virus
(DENV), and West Nile virus (WNV). It is a single-strand-
ed positive RNA virus (10,794-nt genome) that is closely
related to the Spondweni virus and is transmitted by many
Aedes spp. mosquitoes, including Ae. africanus, Ae. lu-
teocephalus, Ae. hensilli, and Ae. aegypti. The virus was
identifie
d
in rhesus monkeys during sylvatic yellow fever
surveillance in the Zika Forest in Uganda in 1947 and was
reported in humans in 1952 (1).
In 2007, an outbreak of ZIKV was reported in Yap Is-
land, Federated States of Micronesia (2). ZIKV also caused
a major epidemic in the French Polynesia in 2013–2014 (3),
and New Caledonia reported imported cases from French
Polynesia in 2013 and reported an outbreak in 2014 (4).
A new challenge has arisen in Brazil with the emer-
gence of ZIKV and co-circulation with others arboviruses
(i.e., DENV and chikungunya virus [CHIKV]). We report
ZIKV infection in Brazil associated with a recent ongoing
outbreak in Camaçari, Bahia, Brazil, of an illness charac-
terized by maculopapular rash, fever, myalgias/arthralgia,
and conjunctivitis.
On March 26, 2015, serum samples were obtained
from 24 patients (Table) at Santa Helena Hospital in Cama-
çari who were given a presumptive diagnosis of an acute
viral illness by emergency department physicians. These
patients were given treatment for a dengue-like illness, and
blood samples were obtained for complete blood counts
and serologic testing by using an ELISA specific for IgG
and IgM against DENV.
Serum samples were analyzed at the Federal Univer-
sity of Bahia by reverse transcription PCR (RT-PCR) to
detect DENV, CHIKV, WNV, Mayaro virus, and ZIKV.
In brief, serum samples were subjected to RNA extrac-
tion by using the QIAamp Viral RNA Mini Kit (QIAGEN,
Hilden, Germany). RNA was reverse transcribed by using
the SuperScript II Reverse Transcription Kit (Invitrogen,
Carlsbad, CA, USA) and subjected to PCRs specific for
DENV (5) CHIKV (6), WNV (7) and Mayaro virus (8).
A positive RT-PCR for a partial region of the envelope
gene with primers ZIKVENF and ZIKVENVR (positions
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 10, October 2015 1885
LETTERS
8/25 muestras BA
(Campos G)
8/21 muestras RN
(Zanluca C)
Abril
2015

NEUROTROPISMO
Noviembre de 2013 y febrero de 2014: 72 casos de
complicaciones neurológicas (Cinco en el año anterior)
Antecedente de infecciones compatibles con el Zika
42 casos de síndrome de Guillain-Barré (SGB)
Ioss S. Medecine et maladies infectieuses 44 (2014) 302–307
Dick GW, et al (1952). Estudio en modelo animal-Zika:
La inoculación de algunos ratones demostró debilidad motora, paralisis de los miembros y
muerte posterior; sin embargo, eventualmente, algunos se recuperaron.
Se analizaron los riñones, pulmones, hígado, bazo y cerebro de los ratones.
En ningún otro órgano, fuera el cerebro, el vírus se encuentra presente en cantidades
demostrables.
Edemas generalizados fueron observados en los cerebros de algunos ratones;
degeneración neuronal e infiltración celular también fueron detectados.
Carlos Brito UFPE

CASOS NEUROLÓGICOS CONFIRMADOS EN PERNAMBUCO LCR Y SUERO LAVITE - LABORATORIO DE VIROLOGÍA Y TERAPIA EXPERIMENTAL (FIOCRUZ-PE)
01 caso meningoencefalitis 90 casos en investigación (LCR y suero almacenados)
Apenas 01 caso sin rash (Fiebre+artralgia+edema) Tiempo entre la enfermedad y la alteración neurológica: 3-13 días PCR positivo en muestras tardías
Cuadro neurológico
posterior
Zika (días)
Tiempo entre CV y
muestra positiva PCR
7 27
5 25
5 34
3 27
13 15
4 31
Iniciales
Diagnósticos
Tratamiento
Evolución Inmediata
Evolución despúes de 3 meses
MCSXS ADEM (NMO like) MTP + IGIV incompleta secuela motora MMII y visual bilateral
GGS SGB IGIV incompleta secuela motora en MMII
ACSL SGB IGIV completa
EBS SGB IGIV incompleta secuela motora en los cuatro miembros
MLGS ADEM MTP incompleta secuela motora en los cuatro miembros y declive cognitivo
JLBA SGB IGIV incompleta secuela motora en los cuatro miembros
Leyenda: SGB – Síndrome de Guillain-Barré NMO like: similar a neuromielitis óptica IGIV: inmunoglobulina intravenosa
ADEM: encefalomielitis aguda diseminada MTP: metilprednisolona intravenosa MMII: miembros inferiores

06 pacientes
PCR-Zika positivo: 04 en sangre y 06 en orina
Orina con carga viral más elevada que en las muestras de suero
Las muestras de orina dieron positivo más de 20 días despúes que la viremia
alcanzó un nivel indetectable
Conclusión: ZIKV ARN es detectable en la orina, con una carga más elevada y
con una mayor duración que en el suero.
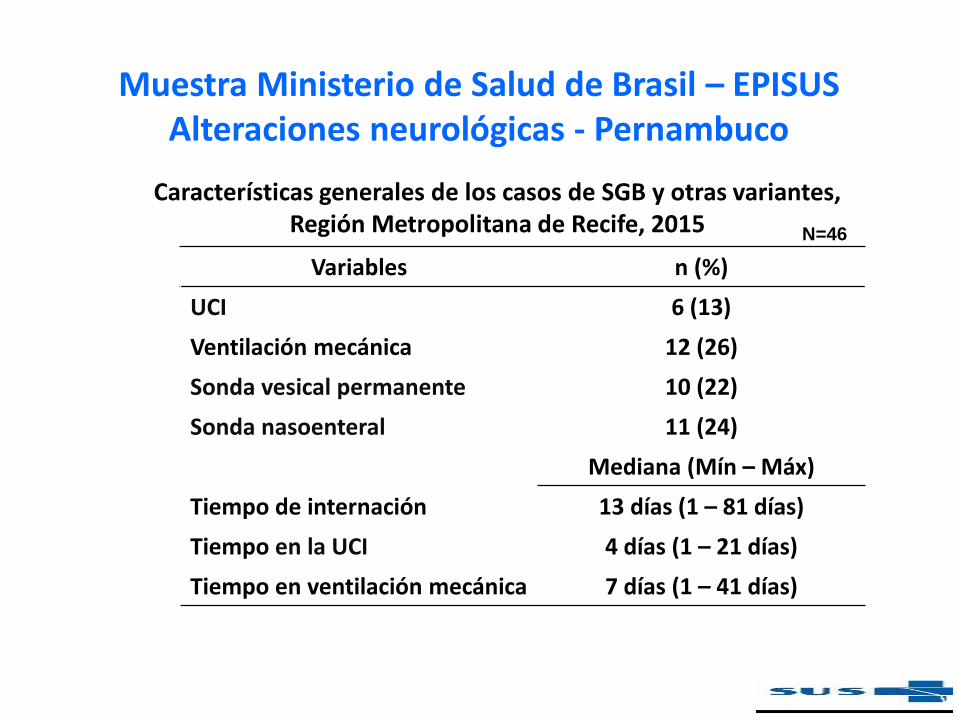
Muestra Ministerio de Salud de Brasil – EPISUS Alteraciones neurológicas - Pernambuco
Características generales de los casos de SGB y otras variantes, Región Metropolitana de Recife, 2015
Variables n (%)
UCI 6 (13)
Ventilación mecánica 12 (26)
Sonda vesical permanente 10 (22)
Sonda nasoenteral 11 (24)
Mediana (Mín – Máx)
Tiempo de internación 13 días (1 – 81 días)
Tiempo en la UCI 4 días (1 – 21 días)
Tiempo en ventilación mecánica 7 días (1 – 41 días)
N=46

Distribución de los casos de SGB y variantes según la evolución, región metropolitana de Recife, 2015
Variables n (%)
Evolución
Cura con secuelas 19 (54)
Cura 20 (30)
Decesos 7 (16)
N=46
Muestra del Ministerio de Salud de Brasil – EPISUS Alteraciones neurológicas - Pernambuco

¿HAY MUCHO POR ELUCIDAR?
Ene Feb Mar Abr May Jun Jul Ago Set Oct Nov Dic
73
164
303
182
Jan Fev Março Abril
Ep
ide
mia
de
Zik
a
Epid
em
ia d
e Z
ika
Zik
a
Epid
em
ia d
e
Zik
a
Estándar de brote de casos neurológicos
1 El tiempo entre la manifestación clínica del Zika y el aparecimiento de los cuadros neurológicos
es más corto que el esperado en muchos casos
Hipótesis: puede haber un efecto citopático directo producido por el vírus, más allá del
inmunomediado (Dos picos de casos)
2 Hipótesis: ¿Los casos neurológicos y el SGB son más graves en el Zika?
El estudio de caso, el control, podrá ofrecer una respuesta.
Ep
ide
mia
de
Zik
a
Neu
ro
Neu
ro
Neu
ro
Ene Feb
Neu
ro
Ep
idem
ia d
e Z
ika
Ep
idem
ia d
e Z
ika
Neu
ro
Neu
ro
Ep
ide
mia
de
Zik
a
Neu
ro

Puntos relevantes:
41 casos serología Zika IgM
Controles de la población general (n: 98): 17% IgM positivo
PCR todos negativos para los casos de SGB
Progresión rápida para el cuadro neurológico posterior al Zika
(6 días)

MICROCEFALIA – VISIÓN DE LA ASISTENCIA
19/10/15
19/10/15
Neurólogo= relato
de aumento
microcefalia.
Se solicita la
opinión del clínico
por su experiencia
en brotes
20/11/15. Visita al IMIP
Dra. Jucile Menezes.
16 niños internados
con microcefalia
“Los especialistas
nunca vieron un
número tan elevado de
casos en tan poco
tiempo" = esto de por
sí supone una
investigación.
Se efectuaron
entrevistas con las
madres, se tomaron
muestras de suero
(madres-niños) y LCR.
La historia clínica
epidemiológica = Zika
Se formula hipótesis
20/10/15
CONSIDERACIONES - ARBOVIROSIS
Sugerimos la arbovirosis, como uno de los posibles agentes que deben ser
investigados y como principal hipótesis, baseados en los seguintes
argumentos:
Aparecimiento de muchos casos, en poco tiempo, simultáneamente en
diferentes ciudades y estados, se caracteriza por ser una enfermedad con
altas tasas de ataques y rápida diseminación, fenómeno asociado a
enfermedades transmitidas por artrópode.
Enfermedades asociadas a TORCH, incluyendo CMV, por las vías de
transmisión, no está asociado a grandes brotes, ni ocurren
simultáneamente en diferentes ciudades.
La investigación durante el prenatal y el perinatal arrojaron resultados
negativos para TORCH en los primeiros casos.
Por el tipo de malformación, la exposición debe haber ocurrido en el primer
trimestre del embarazo.
Carlos Brito UFPE

CONSIDERACIONES - ARBOVIROSIS
La mayoría de las madres (63%) relatava haber tenido un cuadro viral compatible con
enfermedad exantemática en el primer trimestre de 2015.
Tuvimos en Pernambuco, en el primer semestre, un gran brote de virus Zika.
El Zika tiene un neurotropismo mayor que en otras arbovirosis. (Demostrado en modelo
animal y sospechoso en la Polinesia Francesa) y confirmado en Pernambuco.
El Ministerio de Salud de Brasil investiga en este momento casos neurológicos en adultos
y niños, asociados al ZikV, en otros estados.
Otras arbovirosis como el Dengue, endémica y epidémica en la región, no están
asociadas a malformaciones congénitas (7), en la chikungunya, pese a estar relacionada
a enfermedad perinatal, no hay evidencias de malformaciones (8), bien así como el ChikV
aun no había sido detectado en estos dos estados a principios de año.
Carlos Brito UFPE/Fiocruz-PE

Variable
Edad (años) Mediana (Intervalo)
23 (15 - 38)
Síntomas n (%)
Exantema 24 (63,2)
Tipo Difuso 18 (75)
Fiebre 11 (45,8)
Artralgia 08 (33,3)
Edema 02 (8,3)
Conjuntivitis 0 (0)
Resultados preliminares - Caso Microcefalia N=38
Carlos Brito UFPE

Variable
Exantema Mediana (Intervalo)
Periodo de embarazo 3 (1 - 4)
Resultados preliminares - Caso Microcefalia N=24
1
6
14
1
0
2
4
6
8
10
12
14
16
1 mês 2 mês 3 mês 4 mês
M E S D E G E STAC IÓ N D E L
R E L ATO D E E X A NT EMA
58%
21%
Carlos Brito UFPE

MALFORMACIONES DEL SN – ESTACIONALIDAD
PERNAMBUCO
Jan Fev Marc Abril Maio Junh Julho Agost Set Out Nov Dez
2011 9 6 13 11 3 6 7 5 9 12 3 2
2012 4 8 13 7 6 6 5 14 9 3 6
2013 3 8 7 7 10 5 8 15 4 6 4 6
0
2
4
6
8
10
12
14
16
N c
aso
s
Todas Malformaciones Congénitas/
año/mes-PE
2011 2012 2013
Malformações SNC 86 88 83
80
82
84
86
88
Tít
ulo
de
l E
je
Malformaciones Congénitas
del Sistema Nervioso/año-PE
2011 2012 2013 2014 2015
N casos Microcefalia 5 9 10 12 58
0
10
20
30
40
50
60
70
N c
aso
s
N casos Microcefalia
Carlos Brito UFPE

INVESTIGACIÓN– AMPLIA
Epidemias ocasionadas por la introducción de nuevos
teratógenos en la historia:
misoprostol (Cytotec) (Castilla y Orioli, 1994; Orioli y Castilla,
2000),
talidomida (Castilla et al., 1996; Schuler-Faccini et al., 2007),
contaminantes ambientales con ac ción geográficamente
localizada, por ejemplo:
• Cubatão (SP) en 1978 (Monteleone-Neto y Castilla, 1994),
• Goiânia (GO) (Nenot, 1990) en 1987 y
• Caçapava (SP) (Dutra, 1996) en 1988.
Carlos Brito UFPE

AGENTES INFECCIOSOS
Complejo TORCH
• T- Toxoplasmosis
• O- Otras infecciones (Coxsackie, Sífilis, VZV, VIH, Parvovirus
B19, HBV, LCM)
• R- Rubeola
• C- Citomegalovirus
• H – Herpes simplex 1 y 2
Arbovirosis: Dengue, Chikungunya, Zika, Oropouche, Nilo
Occidental, St. Louis, Rocio, etc.
Nuevas Vacunas de virus introducidas en el país (?)
Carlos Brito UFPE

¿PUEDE SER DENGUE?
Se cuenta con suficientes evidencias de que la enfermedad no causa
malformaciones.
Un cambio de comportamiento (mutación) es poco probable.
Carlos Brito UFPE

¿PUEDE SER CHIKUNGUNYA? Algunas buenas evidencias (suficientes) de que la enfermedad no causa
malformaciones
No tuvimos casos o brotes de chikungunya durante el primer trimestre en
Pernambuco
N: 590 embarazadas infectadas por ChikV
Nuestro estudio no encontró ninguna
evidencia de enfermedad congénita en
recién nacidos vivos asintomáticos
expuestos al CHIKV durante el embarazo
RESEARCH
and the mean acceptance rate was 70% (49/70); 43% (21)
of the women included thought that they had had chikun-
gunya infection during pregnancy compared with 6% (4) of
those not included (p<0.0001). Mean parity (2.1 vs. 2.6; p
= 0.08), mean maternal age (28.6 years vs. 29.1 years; p =
0.70), mean gestational age at delivery (39.1 weeks vs. 38.7
weeks; p = 0.14), and mode of delivery (18% vaginal vs.
17% cesarean; p = 0.87) did not differ between the women
who were or were not included.
Discussion
In this comparative study, we did not observe any ef-
fect of chikungynya infection on pregnancy outcomes ex-
cept for the number of prenatal maternal hospital admis-
sions for chikungunya symptoms. Our study involved a
high proportion of maternity units and births in Réunion.
Women included in the study in April 2006 accounted for
73% (905/1,240) of all live births in Réunion. Systematic
determination of serologic status by identifi cation of spe-
cifi c IgM and IgG confi rmed infection status. All patients
for whom chikungunya infection during pregnancy was un-
certain were excluded. We excluded women who had posi-
tive serologic results but did not report symptoms or have
a positive RT-PCR result because we could not identify the
date of infection. Studies during the outbreak in Réunion
showed that IgM tended to persist for 12 to 24 months and
cannot be used to identify the date of infection (21).
Because inclusion in the study began in April 2006 after
the outbreak had peaked, we could not analyze pregnancies
completed before this date. Therefore, our study does not
describe the consequences of the outbreak on the risk for
miscarriage or preterm delivery during the fi rst quarter of
2006. The study included only pregnancies with outcomes
after that quarter. Most of the women were infected before
422 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 16, No. 3, March 2010
Table 3. Pregnancy outcome according to chikungunya virus infection during pregnancy, Réunion, France, 2006*
CharacteristicInfected,†
no. (%), n = 658 Not infected,‡
no. (%), n = 655 p value Unadjusted OR
(95% CI) Adjusted OR
(95% CI)
Hospital admission during pregnancy
Yes 266 (40.4) 191 (29.2) 1.65 (1.31–2.07) 1.52 (1.18–1.95)
No 392 (59.6) 464 (70.8) <0.0001 1 1
Hospital admission during pregnancy, suspected infection with chikungunya virus excluded
Yes 180 (28.0) 136 (26.1) 0.91 (0.70–1.18) 0.83 (0.62–1.10)
No 464 (72.0) 385 (73.9) 0.48 1 1
Vaginal bleeding during pregnancy
Yes 55 (8.4) 68 (10.4) 0.79 (0.55–1.15) 0.94 (0.63–1.42)
No 596 (91.6) 584 (89.6) 0.22 1 1
Obstetric hemorrhaging
Yes 36 (5.6) 42 (6.5) 0.85 (0.54–1.35) 0.87 (0.53–1.42)
No 609 (94.4) 605 (93.5) 0.49 1 1
Mode of delivery§
Vaginal 545 (83.8) 530 (81.5) 0.27 1 1
Cesarean 105 (16.2) 120 (18.5) 0.85 (0.64–1.14) 0.77 (0.56–1.06)
Mean gestational age, wk§ 39.0 (2.1) 38.9 (2.5) 0.55
<32 8 (1.2) 15 (2.3) 0.26 0.52 (0.22-1.24) 0.48 (0.19–1.23)
32–36 53 (8.2) 60 (9.2) 0.86 (0.59–1.27) 0.78 (0.51–1.20)
>37 589 (90.6) 575 (88.5) 1 1
Mean birthweight, g§ 3,116 (549) 3.056 (620) 0.27
<2,000 20 (3.1) 32 (4.9) 0.36 0.62 (0.35–1.11) 0.66 (0.36–1.22)
2,000–2,999 235 (35.9) 236 (35.7) 0.99 (0.79–1.25) 1.01 (0.79–1.30)
3,000–3,999 372 (56.9) 371 (56.1) 1 1
>4,000 27 (4.1) 22 (3.3) 1.22 (0.69–2.19) 1.25 (0.65–2.39)
Stillbirth after 22 wk§
Yes 5 (0.8) 8 (1.2) 0.63 (0.20–1.93) 0.61 (0.18–2.07)
No 653 (99.2) 656 (98.8) 0.41 1 1
Congenital malformation
Yes 19 (2.9) 15 (2.2) 1.36 (0.68–2.74) 1.54 (0.68–3.49)
No 647 (97.1) 654 (97.8) 0.48 1 1
Admission to neonatal care§
Yes 53 (8.1) 55 (8.3) 0.97 (0.65–1.44) 1.03 (0.67–1.58)
No 605 (91.9) 609 (91.7) 0.88 1 1
*OR, odds ratio; CI, confidence interval. OR was adjusted for center, educational level, body mass index, and maternal age. Women infected before pregnancy were considered not infected during pregnancy. †Of the 658 women who were infected, 650 had delivered a child after 22 weeks; 658 children were delivered by these women. ‡Of the 655 women who were not infected, 650 had delivered a child after 22 weeks; 664 children were delivered by these women. §Miscarriage before 22 weeks was excluded.
RESEARCH
and the mean acceptance rate was 70% (49/70); 43% (21)
of the women included thought that they had had chikun-
gunya infection during pregnancy compared with 6% (4) of
those not included (p<0.0001). Mean parity (2.1 vs. 2.6; p
= 0.08), mean maternal age (28.6 years vs. 29.1 years; p =
0.70), mean gestational age at delivery (39.1 weeks vs. 38.7
weeks; p = 0.14), and mode of delivery (18% vaginal vs.
17% cesarean; p = 0.87) did not differ between the women
who were or were not included.
Discussion
In this comparative study, we did not observe any ef-
fect of chikungynya infection on pregnancy outcomes ex-
cept for the number of prenatal maternal hospital admis-
sions for chikungunya symptoms. Our study involved a
high proportion of maternity units and births in Réunion.
Women included in the study in April 2006 accounted for
73% (905/1,240) of all live births in Réunion. Systematic
determination of serologic status by identifi cation of spe-
cifi c IgM and IgG confi rmed infection status. All patients
for whom chikungunya infection during pregnancy was un-
certain were excluded. We excluded women who had posi-
tive serologic results but did not report symptoms or have
a positive RT-PCR result because we could not identify the
date of infection. Studies during the outbreak in Réunion
showed that IgM tended to persist for 12 to 24 months and
cannot be used to identify the date of infection (21).
Because inclusion in the study began in April 2006 after
the outbreak had peaked, we could not analyze pregnancies
completed before this date. Therefore, our study does not
describe the consequences of the outbreak on the risk for
miscarriage or preterm delivery during the fi rst quarter of
2006. The study included only pregnancies with outcomes
after that quarter. Most of the women were infected before
422 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 16, No. 3, March 2010
Table 3. Pregnancy outcome according to chikungunya virus infection during pregnancy, Réunion, France, 2006*
CharacteristicInfected,†
no. (%), n = 658 Not infected,‡
no. (%), n = 655 p value Unadjusted OR
(95% CI) Adjusted OR
(95% CI)
Hospital admission during pregnancy
Yes 266 (40.4) 191 (29.2) 1.65 (1.31–2.07) 1.52 (1.18–1.95)
No 392 (59.6) 464 (70.8) <0.0001 1 1
Hospital admission during pregnancy, suspected infection with chikungunya virus excluded
Yes 180 (28.0) 136 (26.1) 0.91 (0.70–1.18) 0.83 (0.62–1.10)
No 464 (72.0) 385 (73.9) 0.48 1 1
Vaginal bleeding during pregnancy
Yes 55 (8.4) 68 (10.4) 0.79 (0.55–1.15) 0.94 (0.63–1.42)
No 596 (91.6) 584 (89.6) 0.22 1 1
Obstetric hemorrhaging
Yes 36 (5.6) 42 (6.5) 0.85 (0.54–1.35) 0.87 (0.53–1.42)
No 609 (94.4) 605 (93.5) 0.49 1 1
Mode of delivery§
Vaginal 545 (83.8) 530 (81.5) 0.27 1 1
Cesarean 105 (16.2) 120 (18.5) 0.85 (0.64–1.14) 0.77 (0.56–1.06)
Mean gestational age, wk§ 39.0 (2.1) 38.9 (2.5) 0.55
<32 8 (1.2) 15 (2.3) 0.26 0.52 (0.22-1.24) 0.48 (0.19–1.23)
32–36 53 (8.2) 60 (9.2) 0.86 (0.59–1.27) 0.78 (0.51–1.20)
>37 589 (90.6) 575 (88.5) 1 1
Mean birthweight, g§ 3,116 (549) 3.056 (620) 0.27
<2,000 20 (3.1) 32 (4.9) 0.36 0.62 (0.35–1.11) 0.66 (0.36–1.22)
2,000–2,999 235 (35.9) 236 (35.7) 0.99 (0.79–1.25) 1.01 (0.79–1.30)
3,000–3,999 372 (56.9) 371 (56.1) 1 1
>4,000 27 (4.1) 22 (3.3) 1.22 (0.69–2.19) 1.25 (0.65–2.39)
Stillbirth after 22 wk§
Yes 5 (0.8) 8 (1.2) 0.63 (0.20–1.93) 0.61 (0.18–2.07)
No 653 (99.2) 656 (98.8) 0.41 1 1
Congenital malformation
Yes 19 (2.9) 15 (2.2) 1.36 (0.68–2.74) 1.54 (0.68–3.49)
No 647 (97.1) 654 (97.8) 0.48 1 1
Admission to neonatal care§
Yes 53 (8.1) 55 (8.3) 0.97 (0.65–1.44) 1.03 (0.67–1.58)
No 605 (91.9) 609 (91.7) 0.88 1 1
*OR, odds ratio; CI, confidence interval. OR was adjusted for center, educational level, body mass index, and maternal age. Women infected before pregnancy were considered not infected during pregnancy. †Of the 658 women who were infected, 650 had delivered a child after 22 weeks; 658 children were delivered by these women. ‡Of the 655 women who were not infected, 650 had delivered a child after 22 weeks; 664 children were delivered by these women. §Miscarriage before 22 weeks was excluded.
Mother-to-child transmission of chikungunya virus was
reported during the 2005–2006 outbreak on Réunion Island,
France. To determine the effects of this virus on pregnancy
outcomes, we conducted a study of pregnant women in
Réunion in 2006. The study population was composed of
1,400 pregnant women (628 uninfected, 658 infected during
pregnancy, 27 infected before pregnancy, and 87 infected
on unknown dates). We compared pregnancy outcomes for
655 (628 + 27) women not infected during pregnancy with
658 who were infected during pregnancy. Infection occurred
during the fi rst trimester for 15% of the infected women, the
second for 59%, and the third for 26%. Only hospital admis-
sion during pregnancy differed between infected and unin-
fected women (40% vs. 29%). Other outcomes (cesarean
deliveries, obstetric hemorrhaging, preterm births, stillbirths
after 22 weeks, birthweight, congenital malformations, and
newborn admissions) were similar. This virus had no ob-
servable effect on pregnancy outcomes.
Chikungunya virus infection is transmitted by mosqui-
toes of the genus Aedes. The virus was fi rst isolated in
1952 and is found in eastern Africa, India, and Southeast
Asia. Symptoms of infection are high fever and disabling
muscle and joint pain, often associated with a rash and
mild bleeding. Persons infected usually recover spontane-
ously in several days to a week (1). Fever and arthralgia
may occur for several months or even years (2). Patients are
treated only for their symptoms because there is no specifi c
treatment for the underlying infection (3). Before the recent
outbreak on the island of Réunion, the disease was not con-
sidered life-threatening.
Réunion, a French territory in the southwestern Indian
Ocean, has a population of ≈785,000 inhabitants. Medical
facilities in Réunion are similar to those in mainland France
and other industrialized countries. A major chikungunya
outbreak occurred in Réunion in 2005–2006. At the end of
this outbreak, seroprevalence was estimated to be 38.2%
(95% confi dence interval [CI] 35.9%–40.6%); 300,000
(95% CI 283,000–320,000) persons were infected (4,5).
Aedes albopictus mosquitoes were the primary vector in
this outbreak.
The outbreak began in eastern Africa (6). It reached
Réunion in March 2005 but was relatively inactive, with
only several thousand cases until November 2005, when
its incidence unexpectedly increased during summer in the
Southern Hemisphere, peaking at 47,000 cases/week dur-
ing week 5 of 2006. The most recent cases were reported
in August 2006. Comparisons of 2006 with previous years
showed that mortality rates increased during February,
March, and April 2006 (7,8). Since 2006, the virus has
caused several epidemics in the Indian Ocean region (Mad-
agascar, India, Sri Lanka, Thailand, Malaysia, and Singa-
pore). Three new cases of chikungunya were reported in
August 2009 on Réunion Island (9).
The fi rst cases of virus transmission from mother to
child at birth were identifi ed in February 2006; a total of 38
such cases were reported (10,11). The virus was also found
Chikungunya Virus Infection during
Pregnancy, Réunion, France, 2006
Xavier Fritel, Olivier Rollot, Patrick Gérardin, Bernard-Alex Gaüzère, Jacques Bideault,
Louis Lagarde, Barbara Dhuime, Eric Orvain, Fabrice Cuillier , Duksha Ramful, Sylvain Sampériz,
Marie-Christine Jaffar-Bandjee, Alain Michault, Liliane Cotte, Monique Kaminski,
Alain Fourmaintraux, and the Chikungunya-Mère-Enfant Team
RESEARCH
418 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 16, No. 3, March 2010
Author affi liations: Centre Hospitalier Régional de la Réunion, Saint-
Denis, France (X. Fritel, P. Gérardin, B.-A. Gaüzère, E. Orvain, F.
Cuillier, D. Ramful, S. Sampériz, M.-C. Jaffar-Bandjee, A. Michault,
L. Cotte, A. Fourmaintraux); Centre d’Investigation Clinique–Epi-
démiologie Clinique de la Réunion, Saint-Denis (O. Rollot, P. Gé-
rardin); Institut National de la Santé et de la Recherche Médicale,
Villejuif, France (X. Fritel, P. Gérardin, M. Kaminski); Centre Hos-
pitalier Intercommunal de Saint-Benoit-Saint-André, Saint-Benoit,
France (J. Bideault); Centre Hospitalier Gabriel-Martin, Saint-Paul,
France (L. Lagarde); Clinique Sainte-Clotilde, Saint-Denis (B. Dhu-
ime); and Université Pierre et Marie Curie 6, Paris, France (X. Fri-
tel, P. Gérardin, M. Kaminski)
DOI: 10.3201/eid1603.091403
Chikungunya Virus during Pregnancy
in specimens from 3 early second trimester miscarriages
(12). When this outbreak began, little information was
available about the risk for chikungunya virus infection in
pregnant women. In addition to virus transmission at birth,
potential complications include transplacental transmission
before birth, congenital malformations, stillbirths, growth
restriction, and preterm delivery. Chikungunya virus be-
longs to the same family of viruses (Togaviridae) as rubella
virus, for which some of these complications have been de-
scribed (13). The high fever that characterizes chikungu-
nya infection could cause uterine contractions or fetal heart
rate abnormalities, which might promote spontaneous or
induced preterm delivery (cesarean for fetal salvage). The
hemorrhagic syndrome described at the onset of infection
might be manifested by vaginal bleeding during pregnancy
or third-stage hemorrhaging, as reported for infection with
dengue virus (14,15). The proportion of symptomatic and
asymptomatic infections was also unknown.
The purpose of our study (the Chikungunya-Mère-
Enfant cohort study) was to determine the consequences of
chikungunya infection on pregnancy outcomes. These re-
sults will be useful to public health offi cials and physicians
who provide care for pregnant women or newborns because
chikungunya can be imported by international travelers and
the location of Ae. albopictus mosquitoes has extended be-
yond the tropics (16). These mosquitoes are found in 26
states in the United States and several countries in Europe,
where outbreaks are possible (17,18).
Methods
We began our study in early April 2006, by planning
to recruit all pregnant women (with or without symptoms
of chikungunya infection) who received care at 1 of the 6
main maternity units in Réunion. These 6 units accounted
for 78% of 14,077 live births in Réunion in 2006. Inclusion
in the study was proposed regardless of the reason for a vis-
it or admission. We had planned to include 3,600 women so
that suffi cient children with in utero chikungunya infection
were available to study their psychomotor development. To
show a difference of 10 points in the developmental quo-
tient at 24 months of age, it would have been necessary to
observe 19 children infected in utero. However, because of
the decrease in the outbreak after June 1, we revised our
sample size and included only pregnant women who re-
ported clinical signs suggestive of this infection. The study
cohort was composed of 1,400 pregnant women (mean
term 32 weeks); 1,384 (99%) gave birth in 1 of the 6 partic-
ipating maternity units. Information on pregnancy outcome
for 16 women lost to follow-up was obtained by contacting
each one directly. A total of 914 participants were included
in April, 386 in May, 88 in June, 5 in July, 2 in August, 4 in
September, and 1 in November. In an ancillary study, for 3
days in May 2006, all women who gave birth in the 6 par-
ticipating units were interviewed to determine how women
in the study cohort differed from those not in the study in
terms of chikungunya symptoms, parity, age, gestational
age of the infant at birth, and mode of delivery.
Serologic status for chikungunya virus infection was
determined at participant’s inclusion in the study. All re-
ports of chikungunya fever were confi rmed by using se-
rologic testing or detection of the viral genome in any
specimen by using real-time reverse transcription–PCR
(RT-PCR) (19,20). Serologic tests with negative results
at inclusion were repeated at delivery or when symptoms
suggestive of infection appeared. Histologic examinations
were performed on placentas of all women who had chi-
kungunya infection during pregnancy. RT-PCR was also
performed for placenta and amniotic fl uid samples from
women with symptoms at delivery.
Date of infection was determined by checking patient
history of symptoms or by RT-PCR when available. Wom-
en were classifi ed into 2 groups: those infected by chikun-
gunya virus during pregnancy (symptoms during pregnan-
cy confi rmed by positive serologic or RT-PCR results) and
those not infected (negative serologic results at delivery
or during the preceding 7 days). Women infected before
pregnancy were considered not infected during pregnancy.
We excluded women who were infected but asymptomatic,
those whose symptoms could not be dated, and those with
inconclusive serologic results from analysis.
We analyzed how women infected by chikungunya vi-
rus during pregnancy (658) differed from those who were
not infected (655) for general characteristics (age, educa-
tional level, marital status, and body mass index), medical
history (diabetes and hypertension), and obstetric history
(previous pregnancies, history of preterm delivery, small-
for-gestational-age, or stillbirths). We then compared
pregnancy outcomes (prenatal hospital admission for any
reason and for chikungunya symptoms, vaginal bleeding
during pregnancy, mode of delivery, obstetric hemorrhage,
stillbirth, preterm birth, birthweight, congenital malforma-
tions, and newborn hospitalization) between the 2 groups.
Obstetric hemorrhage was defi ned as blood loss >500 mL.
We considered only fetal malformations recognized by Eu-
ropean Surveillance of Congenital Abnormalities (EURO-
CAT) (www.eurocat.ulster.antibodies.uk). All malforma-
tions recorded were verifi ed by checking either pediatric
fi les or the Réunion congenital anomalies registry, which is
affi liated with EUROCAT.
Bivariate analysis of pregnancy outcomes compared
means (by Wilcoxon rank-sum test) and percentages (χ2 or
Fisher exact tests). For multivariate analysis, we adjusted
for center, maternal age, educational level, and body mass
index. Logistic regression was used to estimate the ad-
justed odds ratios (ORs). A p value <0.05 was considered
signifi cant. Sensitivity analyses were performed to deter-
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 16, No. 3, March 2010 419
Comparamos los resultados del embarazo para 655 (628 + 27), las
mujeres no infectadas durante el embarazo con 658 que fueron
infectadas durante el embarazo.
Conclusión: No hubo diferencia en los desenlaces (partos cesáreos,
hemorragia obstétrica, nacimientos prematuros, natimuertos después de
22 semanas, peso al nacer, malformaciones congénitas, y de admisión
de recién nacidos). No se observaron efectos de este virus en los
resultados del embarazo.

MICROCEFALIA – VISIÓN DE LA ASISTENCIA
19/10/15
19/10/15
Adélia Henriques
(Neuróloga)= relato
de aumento
microcefalia/
enfermedad viral
antecedente.
Se solicita la
opinión del clínico
debido a su
experiencia en
brotes
26/10/15
26/10/15.
Reunión de técnicos
en un consejo
técnico del
CREMEPE –
Multidisciplinar –
debatir protocolos e
impresiones.
Se propone una
amplia investigación.
Zika fuerte candidato
(datos clínico-
epidemiológicos)
11/11/15
11/11/15.
Gobierno
Federal
declara
estado de
emergencia
en la Salud
Publica
22/10/15.
Comunicado al
PNCD
(Claudio
Maierovitch
Giovanine Evelin)
26 casos en 3
maternidades con
caracterización
suficiente para
una notificación
oficial a la OMS
Se elabora
comunicado en
conjunto
asistencia y SSE-
PE, MS.
22/10/15
20/11/15. Visita al IMIP
Dra. Jucile Menezes.
16 niños internados
con microcefalia
“Los especialistas
nunca vieron un
número tan elevado de
casos en tan poco
tiempo" = esto de por
sí supone una
investigación.
Se entrevista a las
madres, se toman
muestras de suero
(madres-niños) y LCR.
Historia clínica de la
infección previa = Zika
Se formula hipotesis
20/10/15
21/10/15
Dra. Kleber Luz-RN
Efectua una búsqueda
activa en la asistencia y
confirma el aumento de
casos con antecedente
compatíble con Zika.
Toma fuerza la hipótesis
de arbovirosis
21/10/15
17/11/15.
Liq Amniótico en
gestantes con
microcefalia en PB
PCR+ para Zika
“Es altamente
probable que el
aumento de casos
esté relacionado con
el Zika”
Claudio Maierovitch
17/11/15

CUESTIONES PERTINENTES
¿POR QUÉ NO SE DETECTARON CASOS DE MICROCEFALIA EN LA POLINESIA FRANCESA?
Hipótesis: enfermedad con tasas de incidencia pequeñas, se necesita un "gran
volumen" para ser percibida.
Referencial: Incidencia estimada de microcefalia por 1.000 NV en Pernambuco, últimos 4 años: 0,05 (2011 a
2014)
Polinesia Francesa
o Población 270.000
o Tasa de natalidad por 1000 hab: 15
o En 2014: alrededor de 4.000 nacidos vivos
o Incidencia estimada de microcefalia 0,05/1000: serían 0.2 casos/año - 01 caso por año
o Si ocurriera un aumento del 500% en la Polinesia, serían 4 casos en un año.
Conclusión: es difícil que la asistencia perciba puntos fuera de la curva, en poblaciones pequeñas y en pequeños
números de nacidos vivos, aunque todos ocurrieran el mismo mes.
Pernambuco:
o 144.000 nacidos vivos por año
o Microcefalia estimada (media): 7 casos por año (osciló de 5 a 12 casos en los últimos 4 años).
o En 2015, en cuanto fue percibida por la asistencia, fueron 28 casos en un único mes
o Otros 20 casos ya habían sido notificados al SINASC, y el sistema no había notado este incremento, pero ya
representaba 100% de aumento: nótese la dificultad para identificar el punto fuera de la curva
o El aumento en escala (28 casos) llevó a la captación a través de la asistencia
Conclusión: las exposiciones con pequeñas tasas de incidencia, que conducen a desenlaces como estos, apenas son
perceptibles en grandes poblaciones, con altas tasas de natalidad

¿ASOCIACIÓN Y PERSPECTIVA?
Ene Feb Mar Abr May Jun Jul Ago Sep Oct Nov Dic M
icro
ce
falia
Mic
roce
falia
73
164
303
182
Jan Fev Março Abril
Ep
ide
mia
de
Zik
a
Epid
em
ia d
e Z
ika
Zik
a
Epid
em
ia d
e
Zik
a
¿Cuándo quedaron embarazadas?
1 Hipótesis: estamos viendo gestantes expuestas en enero/febrero que tuvieron sus bebés en
septiembre/octubre.
Conclusión: Estaríamos entonces en el inicio de la epidemia, ya que en marzo fue el mayor pico y
exposición.
Error: el análisis detectó que estas madres fueron expuestas exactamente en el 3º mes de
embarazo, en consecuencia, estaríamos viendo madres expuestas en el mes de pico de la
epidemia.
2 Hipótesis: madres que estaban en el primer o segundo mes de embarazo en el pico de la
epidemia (marzo), en noviembre y diciembre, fecha prevista para el parto, aparecerán casos en
igual proporción.
¿Estos niños presentarán malformaciones más graves?
3 Hipótesis: una infección congénita asociada a una malformación está relacionada a mayor frecuencia de aborto.
¿Tuvimos un aumento del número de abortos en el primer semestre de este año?
Mic
roce
falia
Mic
roce
falia
Ep
ide
mia
de
Zik
a
Mic
roce
falia
Mic
roce
fal
ia
Ene Feb
Neu
ro
Neu
ro
Neu
ro
Neu
ro
Neu
ro
Neu
ro
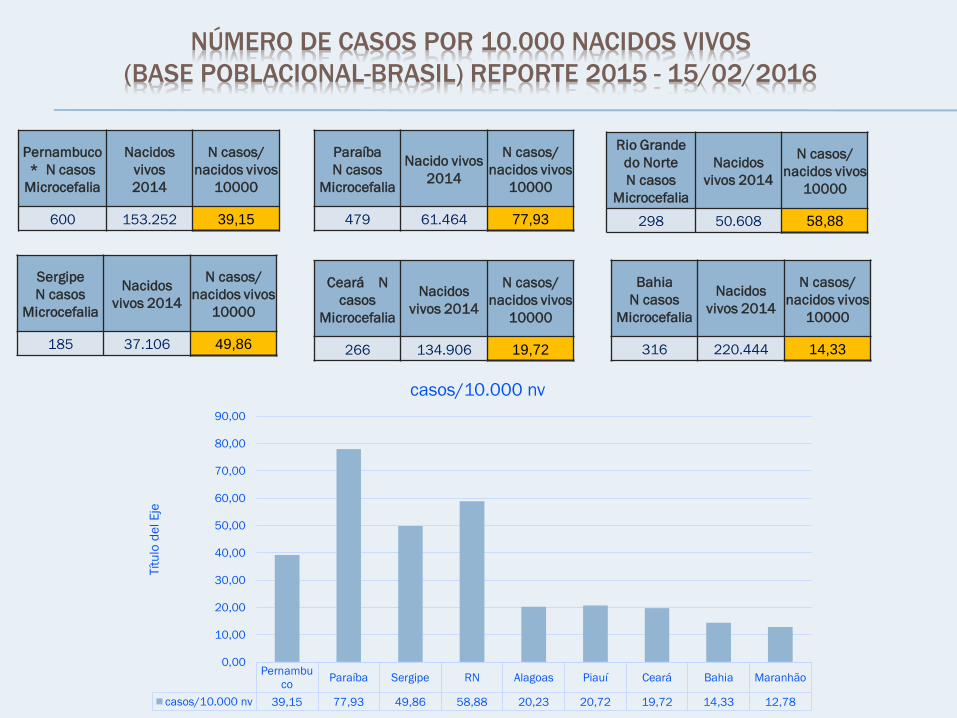
NÚMERO DE CASOS POR 10.000 NACIDOS VIVOS
(BASE POBLACIONAL-BRASIL) REPORTE 2015 - 15/02/2016
Pernambuco
* N casos
Microcefalia
Nacidos
vivos
2014
N casos/
nacidos vivos
10000
600 153.252 39,15
Rio Grande
do Norte
N casos
Microcefalia
Nacidos
vivos 2014
N casos/
nacidos vivos
10000
298 50.608 58,88
Paraíba
N casos
Microcefalia
Nacido vivos
2014
N casos/
nacidos vivos
10000
479 61.464 77,93
Sergipe
N casos
Microcefalia
Nacidos
vivos 2014
N casos/
nacidos vivos
10000
185 37.106 49,86
Bahia
N casos
Microcefalia
Nacidos
vivos 2014
N casos/
nacidos vivos
10000
316 220.444 14,33
Ceará N
casos
Microcefalia
Nacidos
vivos 2014
N casos/
nacidos vivos
10000
266 134.906 19,72
Pernambu
coParaíba Sergipe RN Alagoas Piauí Ceará Bahia Maranhão
casos/10.000 nv 39,15 77,93 49,86 58,88 20,23 20,72 19,72 14,33 12,78
0,00
10,00
20,00
30,00
40,00
50,00
60,00
70,00
80,00
90,00
Tít
ulo
de
l E
je
casos/10.000 nv

INFECCIÓN CONGÉNITA ASOCIADA AL ZIKA
O EL ZIKA CONGÉNITO