
Efectividad del Medicamento en la Práctica Clínica...
37
Efectividad del Medicamento en la Práctica Clínica Outcomes Clínicos en Infección por VIH Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid
Transcript of Efectividad del Medicamento en la Práctica Clínica...

Efectividad del Medicamento en la Práctica Clínica
Outcomes Clínicos en Infección por VIH
Santiago Moreno Hospital Ramón y Cajal. IRYCIS.
Madrid
• Eficacia
• Tolerabilidad
• Toxicidad
• Calidad de vida
Outcomes en Ensayos Clínicos

• Continuos cambios en el manejo clínico y
terapéutico de la infección VIH
• Cambios en los marcadores de respuesta
• Cambios en los métodos de análisis
Eficacia: Introducción
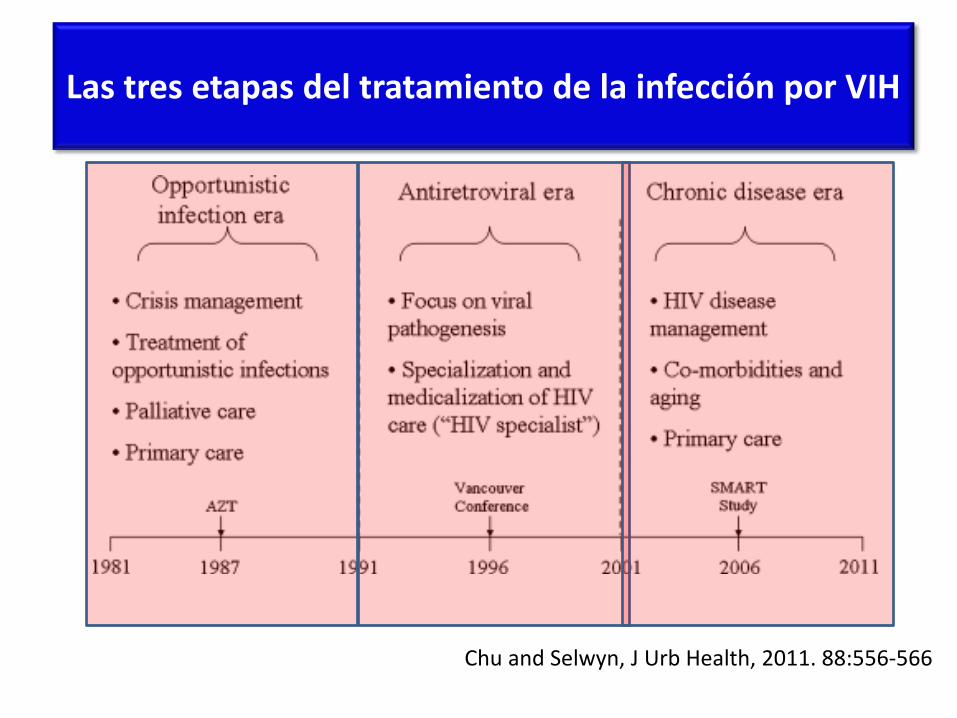
Las tres etapas del tratamiento de la infección por VIH
Chu and Selwyn, J Urb Health, 2011. 88:556-566
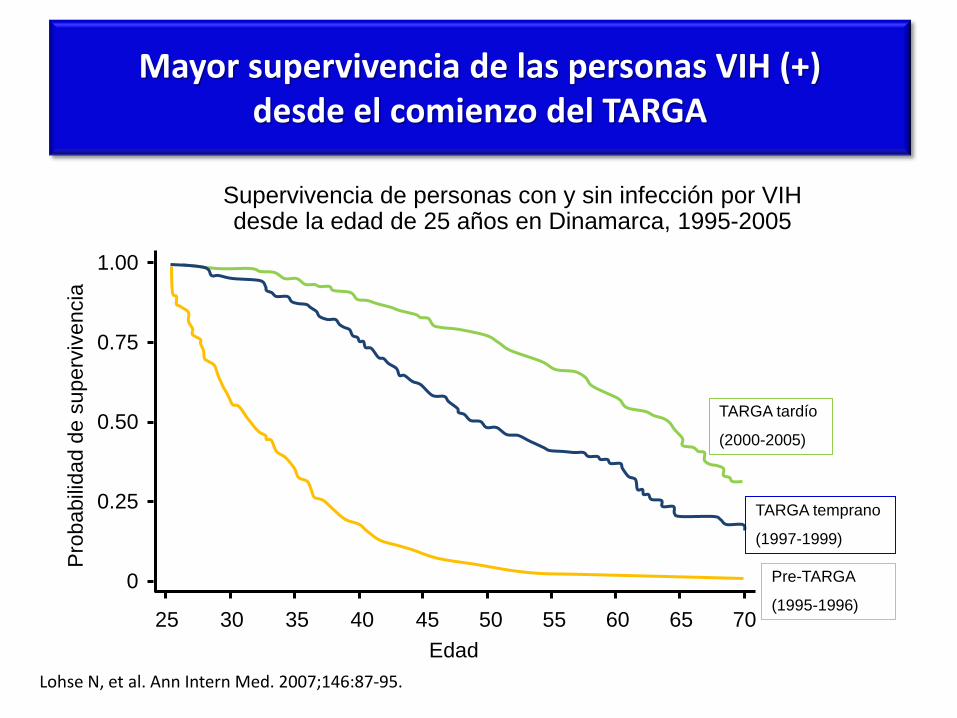
Mayor supervivencia de las personas VIH (+) desde el comienzo del TARGA
Lohse N, et al. Ann Intern Med. 2007;146:87-95.
Pro
babili
dad
de
superv
ivencia
Edad
Pre-TARGA
(1995-1996)
TARGA temprano
(1997-1999)
TARGA tardío
(2000-2005)
Supervivencia de personas con y sin infección por VIH desde la edad de 25 años en Dinamarca, 1995-2005
0
0.25
0.50
0.75
1.00
25 30 35 40 45 50 55 60 65 70
• Epoca inicial: Endpoints “duros”
– Mortalidad
– Progresión a SIDA
– Progresión a SIDA y Mortalidad
Eficacia en Ensayos Clínicos
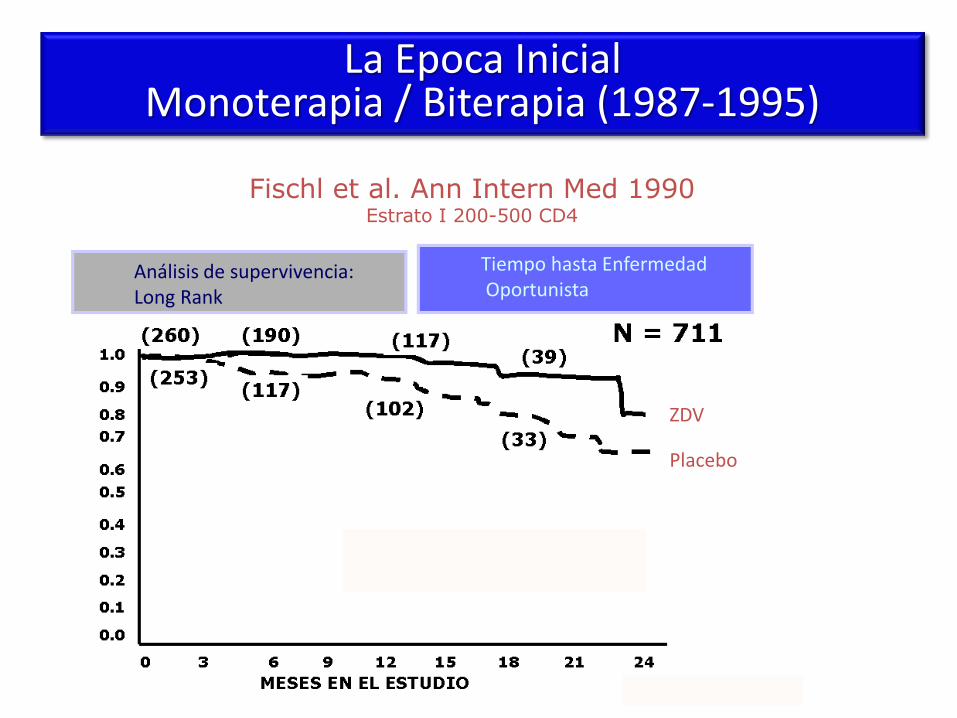
La era de la monoterapia
(1987-1995)
Fischl et al. Ann Intern Med 1990 Estrato I 200-500 CD4
Análisis de supervivencia: Long Rank
Tiempo hasta Enfermedad Oportunista
ZDV
Placebo
La Epoca Inicial Monoterapia / Biterapia (1987-1995)

Mayor supervivencia de las personas VIH (+) desde el comienzo del TARGA
Lohse N, et al. Ann Intern Med. 2007;146:87-95.
Pro
babili
dad
de
superv
ivencia
Edad
Pre-TARGA
(1995-1996)
TARGA temprano
(1997-1999)
TARGA tardío
(2000-2005)
Supervivencia de personas con y sin infección por VIH desde la edad de 25 años en Dinamarca, 1995-2005
0
0.25
0.50
0.75
1.00
25 30 35 40 45 50 55 60 65 70

• Epoca inicial: Endpoints “duros”
– Mortalidad
– Progresión a SIDA
– Progresión a SIDA y Mortalidad
• Epoca intermedia: Marcadores sustitutivos (“surrogate”)
– Recuperación inmunológica
– Reducción de la carga viral
– Pacientes con carga viral indetectable (<200-400 c/mL)
– Mortalidad global
Eficacia en Ensayos Clínicos

Estudio 006 cohorte completa (n= 1266)
<50 copias, IT (perdido = fallo) ICAAC Sep-2000
u
u
u
uu
u
u
u
n
n
n nn
n
n
n
l
l
llll
l
l0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
0 16 24 36 48 60 72Weeks in Study
Pe
rce
nt
of
Pa
tie
nts
N=N=N=
EFV+ZDV+3TCEFV+IDV
IDV+ZDV+3TC
400 401 405 403 405 369417 417 416 418 416 387406 405 402 410 402 390
# Statistically significant difference between EFV+ZDV+3TC and IDV+ZDV+3TC, p 0.05
EFV+ZDV+3TCEFV+IDVIDV+ZDV+3TC

Mayor supervivencia de las personas VIH (+) desde el comienzo del TARGA
Lohse N, et al. Ann Intern Med. 2007;146:87-95.
Pro
babili
dad
de
superv
ivencia
Edad
Pre-TARGA
(1995-1996)
TARGA temprano
(1997-1999)
TARGA tardío
(2000-2005)
Supervivencia de personas con y sin infección por VIH desde la edad de 25 años en Dinamarca, 1995-2005
0
0.25
0.50
0.75
1.00
25 30 35 40 45 50 55 60 65 70
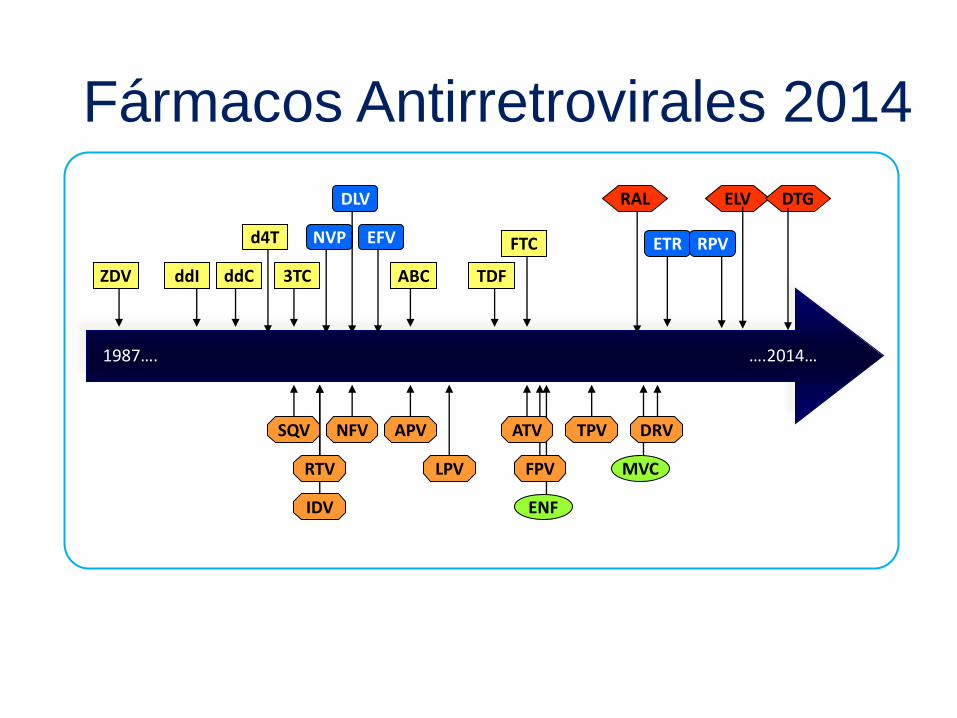
ZDV ddI ddC
d4T
3TC TDF ABC
FTC NVP EFV
DLV
ETR RPV
SQV
RTV
IDV
NFV APV
LPV
ATV
FPV
TPV DRV
RAL
ENF
MVC
ELV
1987…. ….2014…
Fármacos Antirretrovirales 2014
DTG
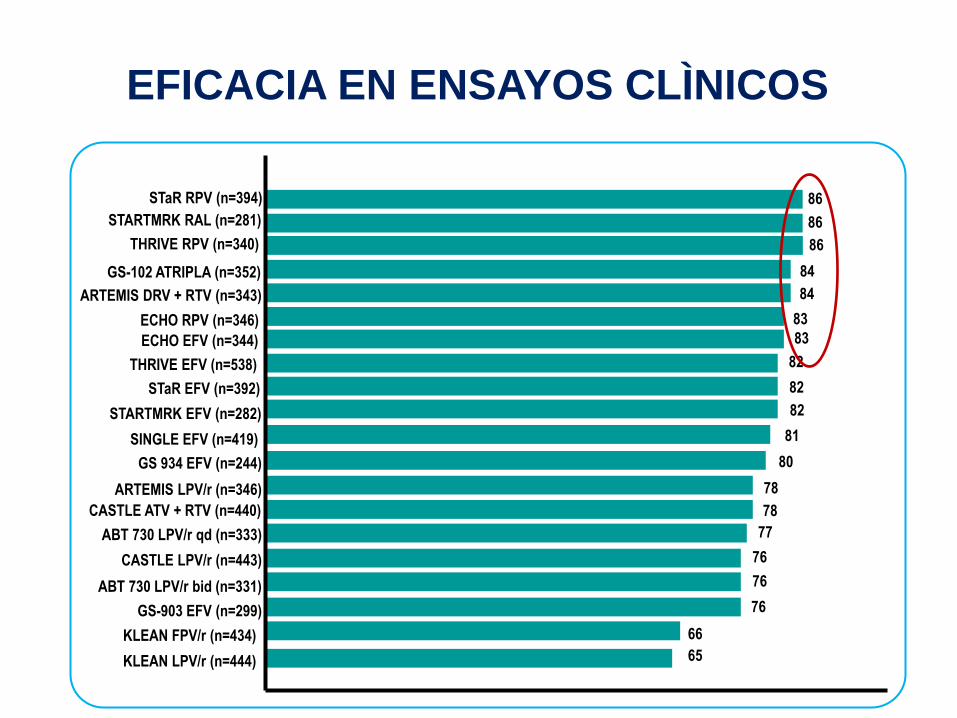
78
77
76
STARTMRK RAL (n=281)
CASTLE ATV + RTV (n=440)
ABT 730 LPV/r qd (n=333)
CASTLE LPV/r (n=443)
84
82 THRIVE EFV (n=538)
76 ABT 730 LPV/r bid (n=331)
86
GS-102 ATRIPLA (n=352)
84 ARTEMIS DRV + RTV (n=343)
83 ECHO RPV (n=346)
76 GS-903 EFV (n=299)
82 STARTMRK EFV (n=282)
80 GS 934 EFV (n=244)
78 ARTEMIS LPV/r (n=346)
82 STaR EFV (n=392)
86 STaR RPV (n=394)
86 THRIVE RPV (n=340)
83 ECHO EFV (n=344)
65 KLEAN LPV/r (n=444)
66 KLEAN FPV/r (n=434)
81 SINGLE EFV (n=419)
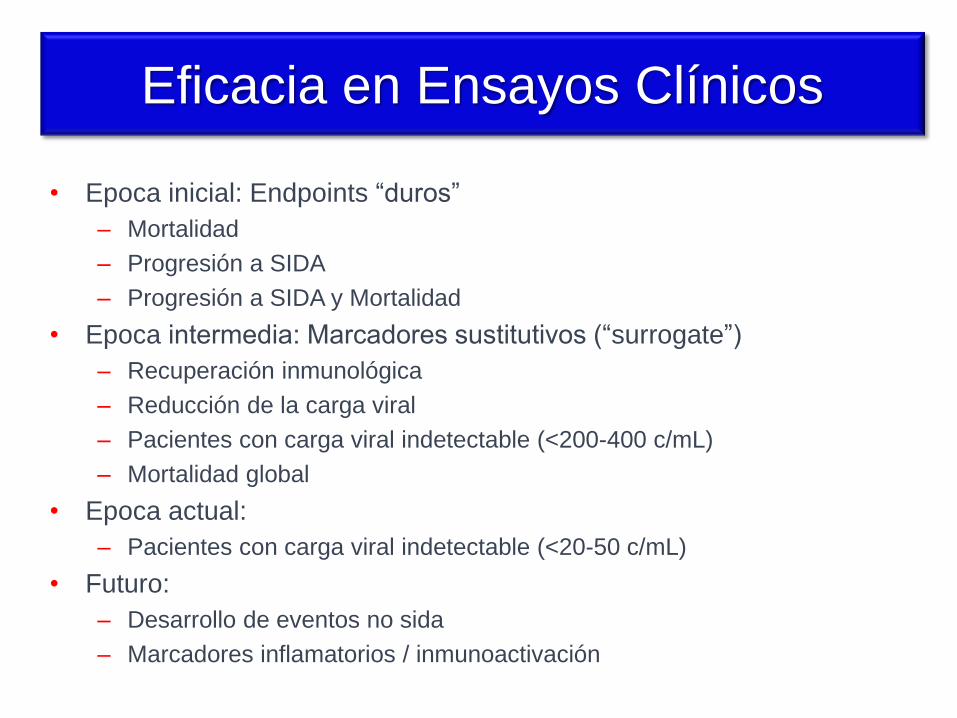
EFICACIA EN ENSAYOS CLÌNICOS
• Epoca inicial: Endpoints “duros”
– Mortalidad
– Progresión a SIDA
– Progresión a SIDA y Mortalidad
• Epoca intermedia: Marcadores sustitutivos (“surrogate”)
– Recuperación inmunológica
– Reducción de la carga viral
– Pacientes con carga viral indetectable (<200-400 c/mL)
– Mortalidad global
• Epoca actual:
– Pacientes con carga viral indetectable (<20-50 c/mL)
Eficacia en Ensayos Clínicos

…pero menor supervivencia que la población general
Lohse N, et al. Ann Intern Med. 2007;146:87-95.
Población general
0
0.25
0.50
0.75
1.00
Edad
25 30 35 40 45 50 55 60 65 70
Pro
babili
dad
de
superv
ivencia
Supervivencia de personas con y sin infección por VIH desde la edad de 25 años en Dinamarca, 1995-2005
TARGA tardío
(2000-2005)
TARGA temprano
(1997-1999)
Pre-TARGA
(1995-1996)

Las enfermedades no relacionadas con el SIDA son responsables del 50% de las muertes en personas VIH+

Activación inmune e inflamación como causas del envejecimiento prematuro
Desai S, Landay A. Early immune senescence in HIV disease. Curr HIV/AIDS Rep. 2010 Feb;7(1):4-10.
• Epoca inicial: Endpoints “duros”
– Mortalidad
– Progresión a SIDA
– Progresión a SIDA y Mortalidad
• Epoca intermedia: Marcadores sustitutivos (“surrogate”)
– Recuperación inmunológica
– Reducción de la carga viral
– Pacientes con carga viral indetectable (<200-400 c/mL)
– Mortalidad global
• Epoca actual:
– Pacientes con carga viral indetectable (<20-50 c/mL)
• Futuro:
– Desarrollo de eventos no sida
– Marcadores inflamatorios / inmunoactivación
Eficacia en Ensayos Clínicos
• Eficacia
• Tolerabilidad
• Toxicidad
• Calidad de vida
Outcomes en Ensayos Clínicos
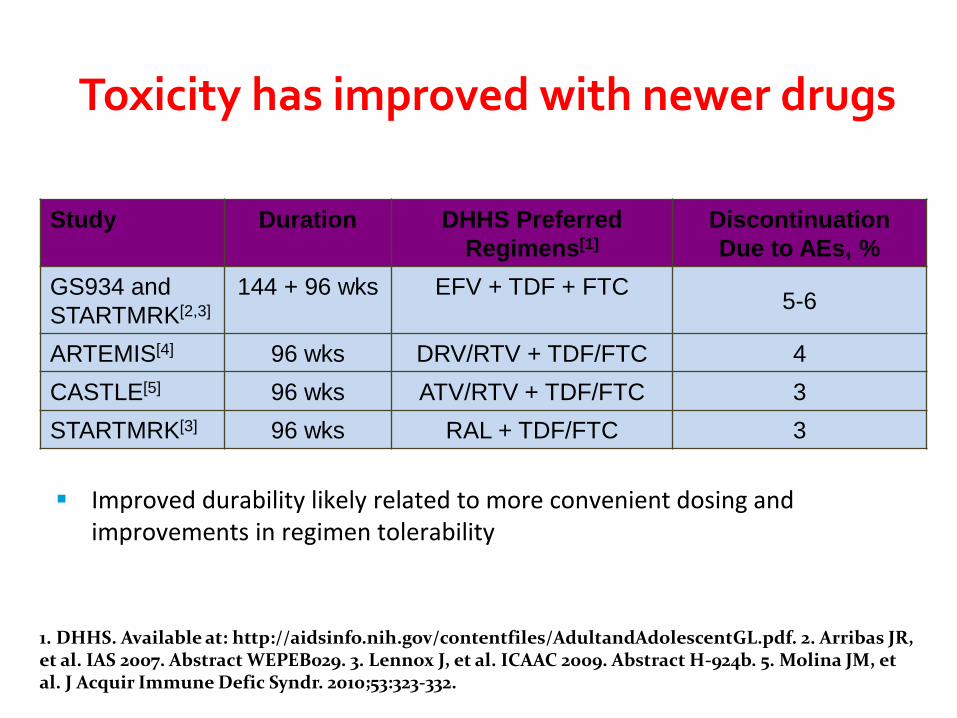
Study Duration DHHS Preferred
Regimens[1]
Discontinuation
Due to AEs, %
GS934 and
STARTMRK[2,3]
144 + 96 wks EFV + TDF + FTC 5-6
ARTEMIS[4] 96 wks DRV/RTV + TDF/FTC 4
CASTLE[5] 96 wks ATV/RTV + TDF/FTC 3
STARTMRK[3] 96 wks RAL + TDF/FTC 3
1. DHHS. Available at: http://aidsinfo.nih.gov/contentfiles/AdultandAdolescentGL.pdf. 2. Arribas JR, et al. IAS 2007. Abstract WEPEB029. 3. Lennox J, et al. ICAAC 2009. Abstract H-924b. 5. Molina JM, et al. J Acquir Immune Defic Syndr. 2010;53:323-332.
Improved durability likely related to more convenient dosing and improvements in regimen tolerability
Toxicity has improved with newer drugs

ACTG 5257: Cumulative Incidence of
Virologic Failure
Difference in 96 wk cumulative incidence (97.5% CI)
-20 0 -10 10 20
3.4% (-0.7%, 7.4%)
5.6% (1.3%, 9.9%)
-2.2% (-6.7%, 2.3%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
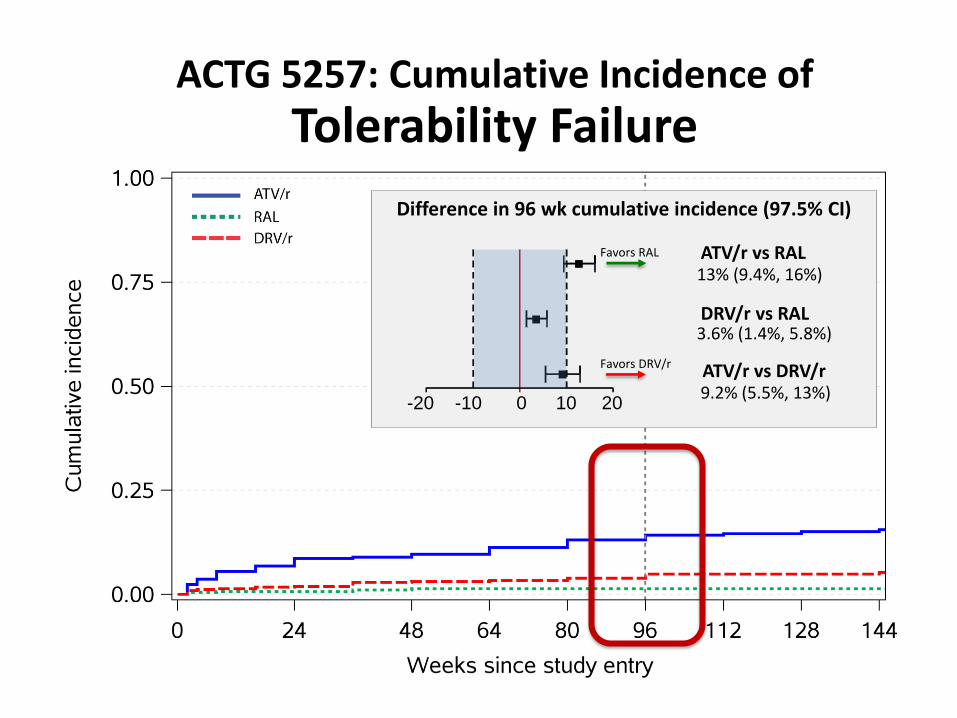
ACTG 5257: Cumulative Incidence of
Tolerability Failure
Difference in 96 wk cumulative incidence (97.5% CI)
-20 0 -10 10 20
13% (9.4%, 16%)
3.6% (1.4%, 5.8%)
9.2% (5.5%, 13%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
Favors RAL
Favors DRV/r

ACTG 5257: Cumulative Incidence of
Virologic or Tolerability Failure
Difference in 96 wk cumulative incidence (97.5% CI)
-20 0 -10 10 20
15% (10%, 20%)
7.5% (3.2%, 12%)
7.5% (2.3%, 13%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
Favors RAL
Favors RAL
Favors DRV/r
*Consistent results seen with TLOVR at a 200 copies/ml threshold
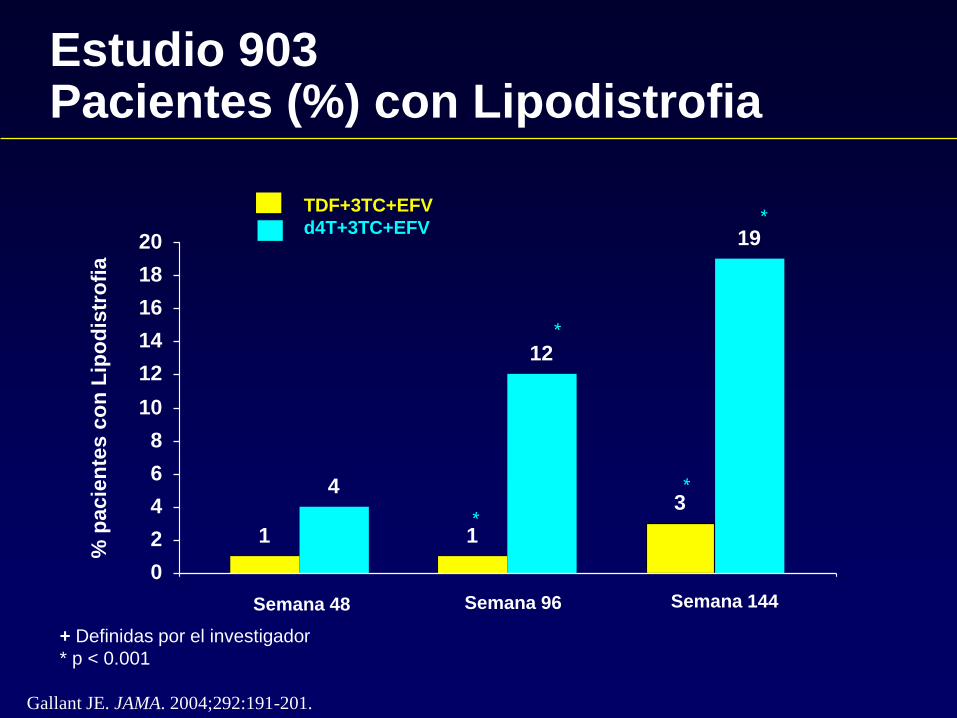
1
4
1
12
3
19
0
2
4
6
8
10
12
14
16
18
20
Estudio 903 Pacientes (%) con Lipodistrofia
% p
acie
nte
s c
on
Lip
od
istr
ofi
a
TDF+3TC+EFV
d4T+3TC+EFV
Semana 48 Semana 96 Semana 144
+ Definidas por el investigador
* p < 0.001
*
*
*
*
Gallant JE. JAMA. 2004;292:191-201.

• Ausencia de diferencias estadísticamente significativas entre los componentes INTI y
los componentes INNTI/IP (prueba de exactitud de Fisher)
Pérdida de grasa (%) de las extremidades entre las semanas 0-96
TDF/FTC
+EFV
(n=56)
TDF/FTC
+ATV/r
(n=45)
ABC/3TC
+EFV
(n=53)
ABC/3TC
+ATV/r
(n=49)
Total
(n=203)
≥ 10%
Principal
14,3%
(6,4%, 25,3%)
15,6%
(7,0%, 28,6%)
18,9%
(9,4%, 31,6%)
16,3%
(7,5%, 28,8%)
16,3%
(11,8%, 22,0%)
≥ 20%
Post hoc
8,9% 0% 3,8% 6,1% 4,9%
Sujetos (%) con una pérdida de grasa en las extremidades ≥10% y ≥20% (análisis ITT, variable principal)
McComsey. et al. 17ª conferencia CROI, San Francisco, CA, 2010, presentación 106LB
Subestudio ACTG 5224

De Jesus E et al. Presented at: 49th ICAAC; September 12-15, 2009; San Francisco, CA. Abstract H-1571.
STARTMRK: Body Composition Changes Through Week 48
0
5
10
15
20
25
30
Appendicular Trunk Total
RAL
EFV
Mea
n (
T/-
SD
) %
Ch
ang
e in
Fat
Co
nte
nt
Fro
m B
asel
ine
16.1 17.4
20.5
17.0 18.0
16.9
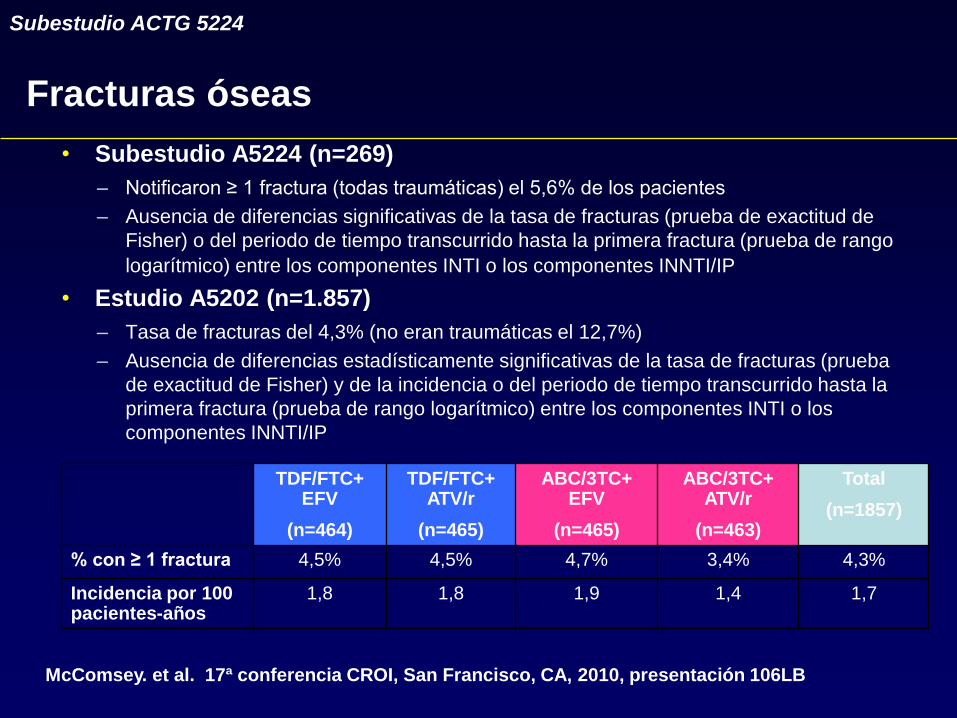
• Subestudio A5224 (n=269)
– Notificaron ≥ 1 fractura (todas traumáticas) el 5,6% de los pacientes
– Ausencia de diferencias significativas de la tasa de fracturas (prueba de exactitud de
Fisher) o del periodo de tiempo transcurrido hasta la primera fractura (prueba de rango
logarítmico) entre los componentes INTI o los componentes INNTI/IP
• Estudio A5202 (n=1.857)
– Tasa de fracturas del 4,3% (no eran traumáticas el 12,7%)
– Ausencia de diferencias estadísticamente significativas de la tasa de fracturas (prueba
de exactitud de Fisher) y de la incidencia o del periodo de tiempo transcurrido hasta la
primera fractura (prueba de rango logarítmico) entre los componentes INTI o los
componentes INNTI/IP
TDF/FTC+ EFV
(n=464)
TDF/FTC+ ATV/r
(n=465)
ABC/3TC+ EFV
(n=465)
ABC/3TC+ ATV/r
(n=463)
Total
(n=1857)
% con ≥ 1 fractura 4,5% 4,5% 4,7% 3,4% 4,3%
Incidencia por 100 pacientes-años
1,8 1,8 1,9 1,4 1,7
Fracturas óseas
McComsey. et al. 17ª conferencia CROI, San Francisco, CA, 2010, presentación 106LB
Subestudio ACTG 5224

Eventos preespecificados
ABC/3TC TDF/FTC
EFV
(n=465)
ATV/r
(n=463)
EFV
(n=464)
ATV/r
(n=465)
Evento cardiovascular, n (%)
vascular*
29 (6)
2 (<1)
29 (6)
2 (<1)
35 (8) 6 (1)
20 (4)
1 (<1)
Neoplasias no SIDA, n (%) 20 (4) 18 (4) 18 (4) 17 (4)
Alteraciones renales, n (%) 12 (3) 14 (3) 5 (1) 12 (3)
Fracturas óseas, n (%) 22 (5) 16 (3) 21 (5) 21 (5)
*Definidos como arteriopatía coronaria, infarto, isquemia, angina, ictus, episodio isquémico transitorio
o enfermedad vascular periférica
Estudio ACTG 5202: atazanavir/r frente a efavirenz – población global
Darr, E. et al., 17ª reunión CROI, San Francisco, CA, 2010, presentación 59LB.
• Eficacia
• Tolerabilidad
• Toxicidad
• Calidad de vida
Outcomes en Ensayos Clínicos
Patient Reported Outcomes
• The following patient reported outcomes may be
collected:
– Adherence by Visual Analog Scale
– Quality of Life (QOL) by SF-36 (v2) survey
– HIV Symptoms Index by a 20-item survey
– Perceived Ease of the Regimen for Condition
(PERC) questionnaire
• Also, a Preference of Medication (POM)
questionnaire may be completed
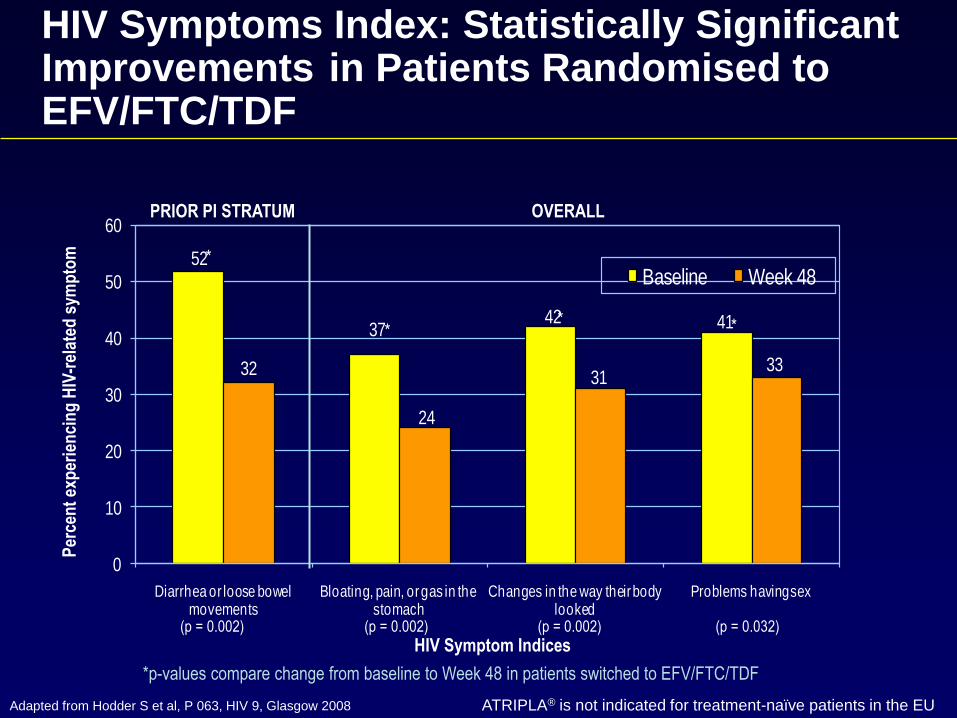
HIV Symptoms Index: Statistically Significant Improvements in Patients Randomised to EFV/FTC/TDF
52
3742 41
32
24
3133
0
10
20
30
40
50
60
Diarrhea or loose bowel movements
Bloating, pain, or gas in the stomach
Changes in the way their body looked
Problems having sex
Baseline Week 48
Per
cen
t ex
per
ien
cin
g H
IV-r
elat
ed s
ymp
tom
HIV Symptom Indices
*p-values compare change from baseline to Week 48 in patients switched to EFV/FTC/TDF
PRIOR PI STRATUM OVERALL
*
* * *
(p = 0.002) (p = 0.002) (p = 0.002) (p = 0.032)
Adapted from Hodder S et al, P 063, HIV 9, Glasgow 2008 ATRIPLA® is not indicated for treatment-naïve patients in the EU
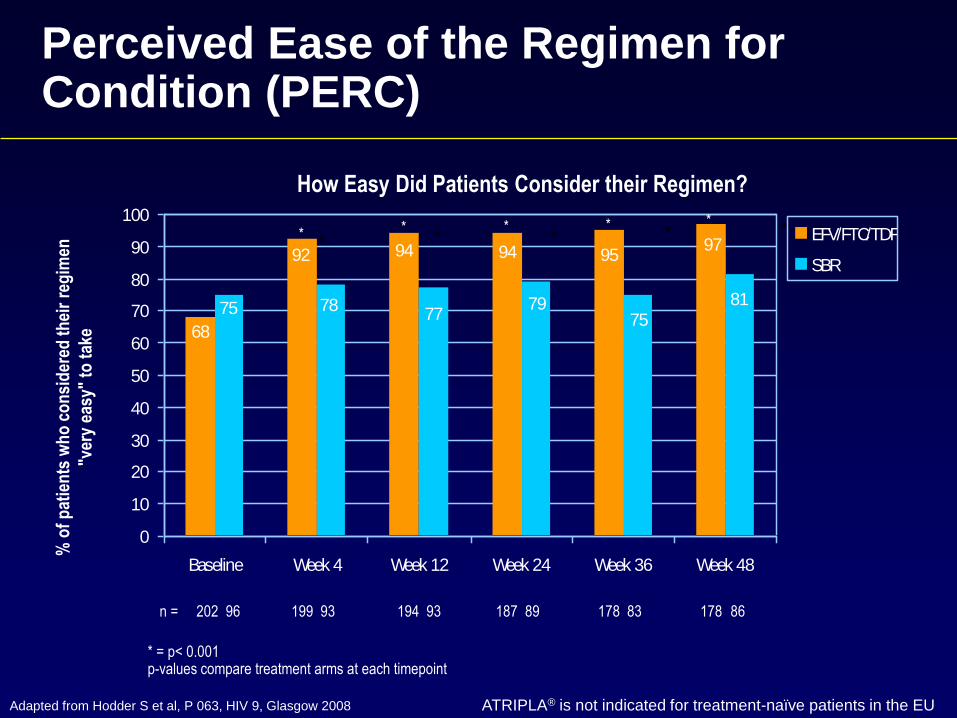
Perceived Ease of the Regimen for Condition (PERC)
% o
f p
atie
nts
wh
o c
on
sid
ered
th
eir
reg
imen
"ver
y ea
sy"
to t
ake
How Easy Did Patients Consider their Regimen?
n = 202 96 199 93 194 93 187 89 178 83 178 86
* = p< 0.001 p-values compare treatment arms at each timepoint
* * * * *
95949492
68
97
8175
7977
7875
0
10
20
30
40
50
60
70
80
90
100
Baseline Week 4 Week 12 Week 24 Week 36 Week 48
EFV/FTC/TDF
SBR
Adapted from Hodder S et al, P 063, HIV 9, Glasgow 2008 ATRIPLA® is not indicated for treatment-naïve patients in the EU
* * * * *
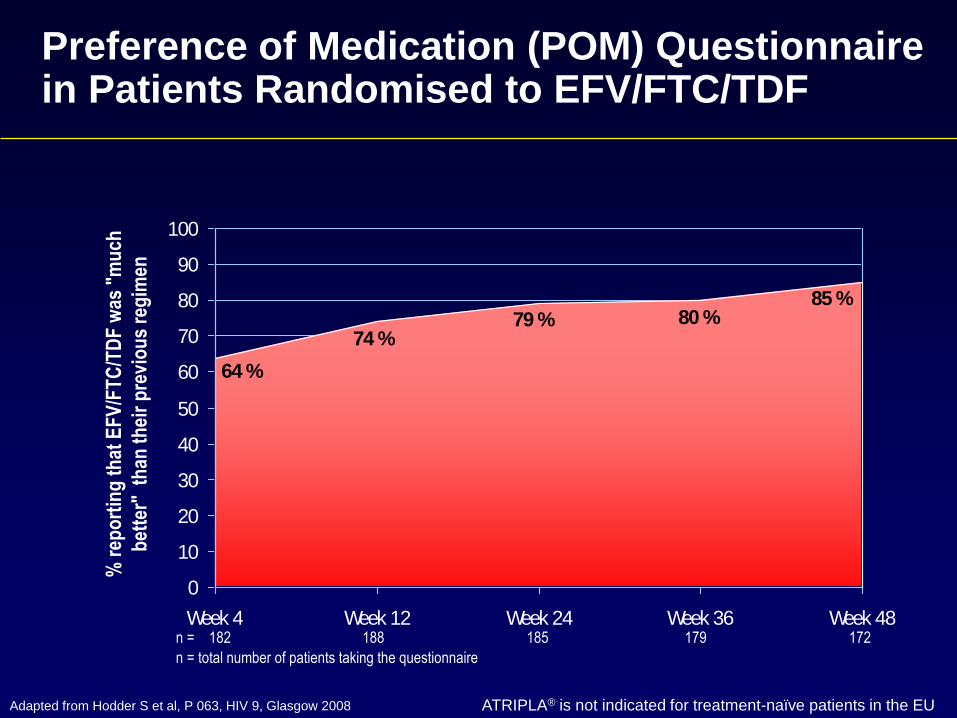
Preference of Medication (POM) Questionnaire in Patients Randomised to EFV/FTC/TDF
64 %
74 %79 % 80 %
85 %
0
10
20
30
40
50
60
70
80
90
100
Week 4 Week 12 Week 24 Week 36 Week 48n = 182 188 185 179 172
n = total number of patients taking the questionnaire
% r
epo
rtin
g t
hat
EF
V/F
TC
/TD
F w
as "
mu
ch
bet
ter"
th
an t
hei
r p
revi
ou
s re
gim
en
Adapted from Hodder S et al, P 063, HIV 9, Glasgow 2008 ATRIPLA® is not indicated for treatment-naïve patients in the EU

• Para tomar decisiones con respecto a tratamiento
antirretroviral se tienen en cuenta resultados
acerca de la eficacia, la toxicidad y el impacto en
la calidad de vida de los fármacos.
• En el momento actual, la mayoría de los
regímenes ofrecen resultados similares en todos
los aspectos y las decisiones pueden venir
condicionadas por otros aspectos (coste).
Outcomes en Infección por VIH

8 años 23 años
39 años*
51 años
*Equivalente a una persona de la misma edad diagnosticada de diabetes
Lohse et al. Ann Intern Med 2007; JAC 2007
Supervivencia a partir de los 25 años
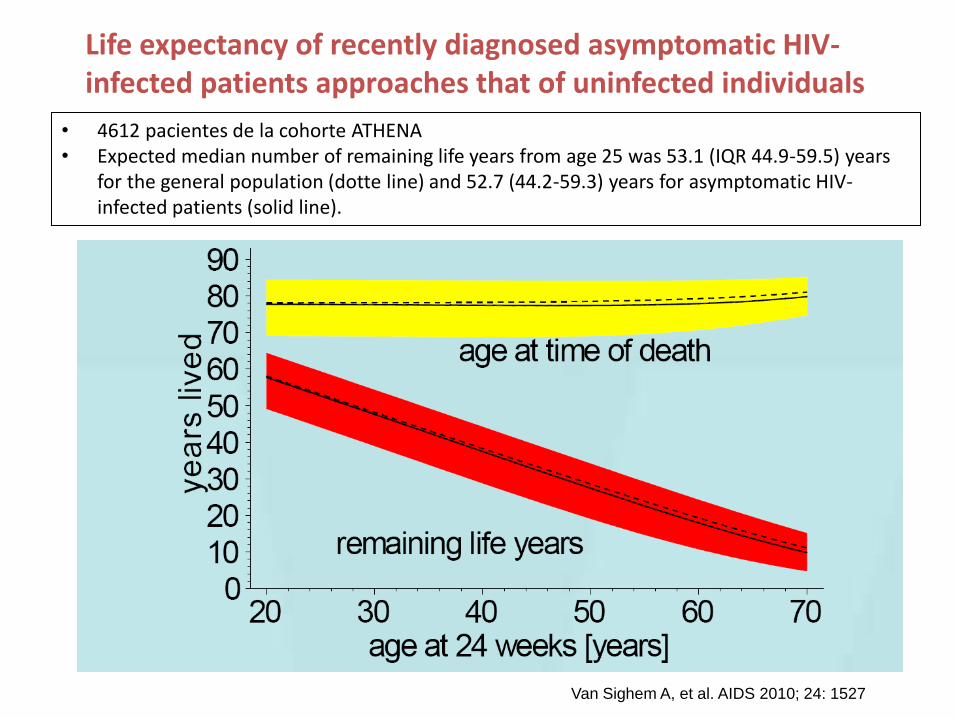
• 4612 pacientes de la cohorte ATHENA • Expected median number of remaining life years from age 25 was 53.1 (IQR 44.9-59.5) years
for the general population (dotte line) and 52.7 (44.2-59.3) years for asymptomatic HIV-infected patients (solid line).
Van Sighem A, et al. AIDS 2010; 24: 1527
Life expectancy of recently diagnosed asymptomatic HIV-infected patients approaches that of uninfected individuals
Muchas Gracias




![*678)-2 )* 9 &/25*6 *1 /& 81-9*56-)&) )* /26 &1 ... - Dialnet · YRTV RUVTeRURc \R ]Rh_bZR UV \Rc `bV(Xe^dRc) 9UVb^Rc5,$ GVb]ZdV YRTVb e^R bR`ZUR T\RcZWZTR(TZ1^ UV \_c VcdeUZR^dVc](https://static.fdocuments.ec/doc/165x107/5e63fb59409d66785739ac13/678-2-9-256-1-81-956-26-1-dialnet-yrtv.jpg)









![µ v ] o À ] µ E } ] , u } } Ç ] ] Ì } ] K v } Z Ç v Z µ u ...5hy ,qy 9hw 3hu~ . %dxwlvwd hw do $%675$&7 7kh remhfwlyh ri wkh suhvhqw vwxg\ zdv wr prqlwru wkh ghwhfwlrq ri wkh](https://static.fdocuments.ec/doc/165x107/5e7e5edb4471f430c71c4b39/-v-o-e-u-oe-k-v-z-v-z-u-5hy-qy-9hw.jpg)



