Cali Cáncer 50 años incidencia & mortalidad RPCC

of 11
-
Upload
fernando-arteaga-suarez -
Category
Documents
-
view
214 -
download
0
Transcript of Cali Cáncer 50 años incidencia & mortalidad RPCC
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
1/11
Available in: http://www.redalyc.org/articulo.oa?id=28324856002
Red de Revistas Cientficas de Amrica Latina, el Caribe, Espaa y Portugal
Sistema de Informacin Cientfica
Bravo, Luis Eduardo; Collazos, Tito; Collazos, Paola; Garca, Luz Stella; Correa, PelayoTrends of cancer incidence and mortality in Cali, Colombia. 50 years experience
Colombia Mdica, vol. 43, nm. 4, octubre-diciembre, 2012, pp. 246-255
Universidad del Valle
Cali, Colombia
How to cite Complete issue More information about this article Journal's homepage
Colombia Mdica,
ISSN (Printed Version): 0120-8322
Universidad del Valle
Colombia
www.redalyc.orgNon-Profit Academic Project, developed under the Open Acces Initiative
http://www.redalyc.org/articulo.oa?id=28324856002http://www.redalyc.org/comocitar.oa?id=28324856002http://www.redalyc.org/fasciculo.oa?id=283&numero=24856http://www.redalyc.org/articulo.oa?id=28324856002http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/articulo.oa?id=28324856002http://www.redalyc.org/revista.oa?id=283http://www.redalyc.org/articulo.oa?id=28324856002http://www.redalyc.org/fasciculo.oa?id=283&numero=24856http://www.redalyc.org/comocitar.oa?id=28324856002http://www.redalyc.org/ -
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
2/11
246
ABSTRACTPurpose :Te Population-based Cancer Registry o Cali aims to report all new cases in permanent residents within the limito the city o Cali. ime trends o cancer incidence and mortality are described. Te registry has been in continuous operationor 50 years.Methods:Cancer cases reports are obtained actively by visiting all sources o inormation: hospitals, pathology departmentshematology laboratories, radiotherapy centers, government offices where death certificates are processed and physicians offices. It is estimated that the reporting is at least 95% complete.Results:Drastic decreases are documented in rates or tumors causally related to inectious agents, especially cancers o theuterine cervix and the stomach. Gradual increases are documented in rates o tumors linked to affluence and the metabolicsyndrome, especially cancers o the colon and the emale breast. An unexpected increase in the incidence o papillary car-cinoma o the thyroid gland in women is reported. obacco-related cancers, especially cancer o the lung, showed markedincrease in incidence rates around 1970, apparently the beginning o an epidemic similar to the one reported in Westernsocieties. But the increase in incidence stopped around 1980, resulting rom a strong anti-smoking campaign launched inColombia in the 1970s.Conclusions:Te findings have influenced prevention strategies implemented by public health authorities, specially the establishment o a city-wide program to prevent cervix cancer via widespread use o vaginal cytology and anti-smoking cam-paigns. Also, new population-based cancer registries have been established in other Colombian cities as well as in Ecuador.
Original Article
Trends of cancer incidence and mortality in Cali, Colombia.50 years experience
Article info
Article history:
Received 2 ebruary 2012Received in revised orm 5 April 2012Accepted 9 September 2012
Keywords:Cancer, epidemiology, Cali, Colombia,cancer trends.
aCancer Registry o Cali, Departament o Pathology. Universidad del Valle, Cali, Colombia
bDivision o Gastroenterology, Department o Medicine, Vanderbilt University Medical Center, Nashville, N, USA.
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
*Corresponding Author.E-mail Address :[email protected](Bravo LE), [email protected] (Collazos p), [email protected] (Garca LE), [email protected] (Correa P ).
Bravo, Luis Eduardoa; Collazos, itoa; Collazos, Paolaa; Garca, Luz Stellaa; Correa, Pelayob.
Colombia Mdicacolombiamedica.univalle.edu.co
Colombia Mdica
Journalhomepage: http://colombiamedica.univalle.edu.co
Facultad de SaludUniversidad del Valle
INTRODUCTION
Reliable data on time trends in cancer incidence and mortality areor the most part unavailable in Latin America. Te main reasonis the scarcity o population-based cancer registries in continuousoperation or prolonged periods o time. Te Population-basedCancer Registry o Cali, Colombia (Registro Poblacional de Can-cer de Cali, RPCC) started 50 years ago as a 2 year incidence sur-
vey. Te objective was to register all new cancer cases diagnosedin the city during 1962 and 1963. Te survey was a joint projecto the departments o Pathology and Preventive Medicine o Uni-
versidad del Valle School o Medicine. A team o medical studentswere especially trained to review and abstract the records o 16medical institutions (1504 hospital beds) and 483 practicing phy-
sicians attending patients in whom cancer could be diagnosedand/or treated. Te survey emphasized registering only new casesin patients who were permanent residents o the city, living withinbounds clearly demarcated by the municipality.
At the time there were no data on cancer incidence in ColombiaData on mortality were unreliable; some death certificates werewritten by non-medical personnel and were not accurate about thecause o death. Some data were available on the relative requencyo cancer in hospitals, but were biased by the selective admissionpolicies o the institution. One study reported relative requencyor all cases diagnosed in the department (state) o Antioquia, based on all histopathology reports or the area 1, 2. Te Cali surveythereore intended to fill the vacuum on inormation about cancerrequency in Colombia. Te results o the survey were publishedin national and international medical journals3-5. Tey revealedhigh rates or cancer o all sites combined, driven in men by gas-tric cancer and in women by carcinoma o the uterine cervix. Telatter was o epidemic proportions. Low rates o colon and lung
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
3/11
247
cancer were reported. Tese findings stimulated urther researchand were instrumental in launching a public health campaign tocontrol cervical cancer, especially by setting up multiple centersor collection o vaginal cytology specimens, processed in a cen-tral laboratory under the direction o a specialized pathologist6. Inthe ollowing years, the rates o carcinoma in situ increased consi-derably and coincided with a decrease in invasive cervical carcino-ma5. Because o the success o the survey, the decision was madeto continue the Registry as a permanent endeavor, based in the
department o Pathology, mostly with resources provided by theUniversity. Systems or capturing the inormation in a permanentbasis were set up in the main institutions, complemented by thehistorically proven successul collaboration o medical students.
THE POPULATION
At that time o the establishment o the Registry the city had578,440 inhabitants; approximately 64% o them were immigrants,mostly rom other regions in Colombia, reflecting economic andpolitical pressures in some rural areas, driving internal migration.A national census was carried out on July 15, 1964. It containeddetailed inormation on the place o birth o each resident. Tisallowed the construction o population pyramids or subjects born
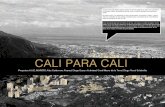
in the city as well as or the main immigrant groups. Tis demo-graphic inormation allowed the calculation o cancer incidencespecific rates or each group o residents7. Population pyramidswere drawn or natives and the main immigrant groups. Te po-pulation o Cali in 1964 displayed a pattern closer to the AricanModel with wide base and narrow apex (Fig. 1). It reflects theinfluence o immigrant s rom rural southern populations (Caucaand Nario) with a typical Arican-type demographic structureand immigration rom urban populations with a pattern closer tothe European model (Bogota and Antioquia)7.Te populationo Cali in 1964 changed into a more European pattern in 2005,when the population had grown to 2,309,626. Te demographicstructure then is seen in Fig. 1. Te aging index (population 65 +
years divided by children under 15 years) is approximately 0.041in 1964 and 0.2472 in 2005. Tereore, the 1964 population wasconsiderably younger than that o 2005. Tese data show a re-markable transormation o the population o Cali in approxima-tely 40 years.
MATERIALS AND METHODS
In 2010 the Registry covered the population o the urban areao Cali with 119 square kilometers. Cali is the capital o the De-
partment (state) o Valle del Cauca, one o the 32 departments inwhich the country is divided politically. Its demographic distri-bution is shown in Fig. 1. Most o the inhabitants are mestizos(ancestral admixture o Amerindians and Caucasian). More thanone hal are immigrants, mostly rom other parts o ColombiaCali is situated 1000 meters above sea level at latitude 3-27 N andlongitude 7-31 W. Te average temperature is 24 degrees Celsius.
Te RPCC is a program o the Department o Pathology o Uni-
versidad del Valle. Cancer cases reports are obtained actively byvisiting all sources o inormation. Tese sources include hospitals, pathology departments, hematology laboratories, radiotherapy centers, government offices where death certificates are processed and physicians offices. It is estimated that the reporting is atleast 95% complete. Standards o quality-control routines, basedon those developed by the International Agency or Research onCancer8are applied to each tumor record. Every two years a groupo specially trained medical students is selected to carry out a fieldsurvey o the files o all private physicians who diagnose or treatcancer patients. More detailed methodology has been previouslypublished5.
Incidence data were obtained rom the Cali Cancer Registry da-tabase and mortality data rom the Cali Municipal Office o VitalStatistics. Te RPCC uses quality assurance procedures, as advocated by IARC, to validate the quality and complementation ocancer registration8. Incidence data and quality indices or these data have been published previously in Cancer Incidence inFive Continents (CI5), Volume I-XII9-16, able 3. For the periodo 2003-2007, the percentage o cases histologically verified was84.5%, the mortality to incidence ratio (M:I) 49.2% and the percentage o records abstracted rom Death certificate only (DCO4.5%. Quality Control or Mortality data: 291725 registries wereanalyzed through 1984-2008, 47034 (16.1%) corresponding tocancer deaths. A high quality index was observed or cancer death
registration with 92.8 % o the cancer deaths properly certifiedTe percent o missing age at death was 0.2%. Te percent o unk-nown and non-specific primary site o cancer was 6.7%. In almosall cases, the death certificates were signed by a physician (99.7%)
Te prevailing International Classification o Diseases (ICD) wasused or cancer classification. Tree ICD versions have been usedthrough the long registration period. Te Eighth Revision, adap-ted or use in the United States, or 1962 to 1978; the Ninth Revi-
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
Figure 1.Cali, Colombia. Population structure by age and sex.
429 85+ 999
581 80 a 84 1011
1159 75 a 79 1641
1732 70 a 74 2629
2799 65 a 69 3542
4825 60 a 64 6281
5776 55 a 59 64178033 50 a 54 9777
10283 45 a 49 11807
13497 40 a 44 14107
17228 35 a 39 19237
20969 30 a 34 23358
22644 25 a 29 27338
25235 20 a 24 3260127138 15 a 19 36844
33210 10 a 14 35228
42935 05 a 09 43435
51910 00 a 04 50780
Females (%)
290383 Total 327032
Males (%)
20% 15% 10% 5% 0% 0% 5% 10% 15% 20%
4128 85+ 7616
5967 80 a 84 9300
11563 75 a 79 16481
15270 70 a 74 21779
20698 65 a 69 28261
25163 60 a 64 32209
33447 55 a 59 42167
43212 50 a 54 54157
54394 45 a 49 67102
67166 40 a 44 79200
70340 35 a 39 81508
71871 30 a 34 81840
79703 25 a 29 82844
85933 20 a 24 9084689341 15 a 19 92206
90365 10 a 14 95340
94953 05 a 09 96286
97949 00 a 04 99021
Females (%)
961463 Total 1078163
Males (%)
20% 15% 10% 5% 0% 0% 5% 10% 15% 20%
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
4/11
248
sion or 1979 to 1998 and the enth Revision or 1998 to 2008. oallow analysis o comparable trends over time, efforts were madeto define the cancer sites consistently over the three editions othe ICD. Te IARCtools program was used in 1998 to convertcodes between ICD versions17. Te main cancer sites were defi-ned according the Global Burden Diseases 2000 classification omalignant neoplasms by site o primary tumor.18 Te NationalAdministrative Department o Statistics in Colombia (DANE)provides the distribution o Cali population according to sex, by5-year age groups. Te DANE has organized five censuses o thetotal Colombian population in 1964, 1973, 1985, 1995 and 200519. Te age-specific person-years were estimated rom these de-cennial census data with exponential interpolation between cen-suses. Age-standardized incidence and mortality rates (ASR) werecalculated by the direct method, using the world standard popu-lation. Rates are expressed per 100,000 person-years20rends oincidence rates were analyzed during nine quinquennial periodsrom 1962 to 2007 and trends o mortality rates were analyzed du-ring five quinquennial periods rom 1984 to 2008. rends o rateswere evaluated by the annual percentage change (APC), using theweighted least squares method embedded in the US National Can-cer Institutes publicly accessible SEER*Stat sofware21Te AnnualPercent Change (APC) represents the average percent increase ordecrease in cancer rates per year over a specified period o time.In describing the change, the terms increase or decrease wereused when the APC was significantly different rom zero (two-sided p values
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
5/11
249
Lung cancer: Incidence and mortality rates are higher in males,p
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
6/11
250
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
Figure 2.Cali, Colombia. rends or cancer incidence rates (1926-2007) and cancer mortality rates (1984-2008).
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
7/11
251
has been generally linked to the gradual decrease in prevalencerates o Helicobacter pyloriinection and the steady improvemento living conditions, including diet and home sanitation. In Co-lombia, the highest incidence rates o gastric cancer are seen inthe Andes Mountains, especially in the southern state o Nario.A positive correlation between altitude over sea level and gastriccancer mortality rates has been reported in Colombia23.
Te highest rates in Cali are seen in immigrants rom Nario 7
It has been reported that in Hawaii, the highest rates are seen inimmigrants rom Japan, but their Hawaiiborn descendents havemuch lower rates24. Te immigrants to Cali themselves have highprevalence o H. pyloriinection but their descendants have verylow inection rates. Te prevalence rates o H. pyloriinection are
very high in Nario but much lower in the inhabitant o the cityo Cali25.It seems reasonable to assume that the chronologic de-crease o gastric cancer rates in Cali is linked to lower H. pyloriinection prevalence rates and improvements in living conditions.It is also probable that the residents o Cali, including the immi-grants, have different dietary patterns that those seen in the ruralAndes Mountains, including lower salt consumption and higherintake o resh ruits and vegetables, known to be associates with
lower cancer rates. Te trends o colorectal cancer incidence andmortality in Cali show a constant steady increase in the 50 yearso observation, first reported in 198322Age-specific rates or malesand emales are practically identical. Tis pattern may reflect thegradual improvement o the socio-economic status o the popula-tion. Te distance between incidence and mortality rates has beenincreasing rom1982 to 1998, suggesting detection at earlier stagesin recent years. In general there is a positive correlation betweencolorectal cancer and socioeconomic status. Low residue and highat diet have been implicated.
Te causal association between lung cancer and tobacco smokinghas been well documented worldwide. Lung cancer incidence ra-
tes or both sexes in Cali can be interpreted as reflecting the abor-ting o a smoking related epidemic that started around 1970 butwas interrupted around 1980. It seems sae to conclude that thisphenomenon is related to a very strong anti-smoking campaignthat has taken place in Colombia since around the 1970s. Mortali-ty rates, available since 1982, never reached epidemic proportionsand show a slight decline since around 1992. Tat campaign seemsto have avoided a major health burden or the Colombian popula-tion. A similar pattern has been reported in other Latin Americancountries, such as Ecuador and Venezuela26and has been linked toanti-smoking campaigns27.
Breast cancer incidence rates, both pre- and post-menopausalshow a steady increase since 1964 which became accentuatedaround 1992. Te same trend has been reported in other LatinAmerican countries, contrasting with decreasing trends in U.S.Aand Canada26. Mortality rates show a very modest increase bet-ween 1982 and 1998; afer that date no urther increase is obser-
ved. As in the case o colon cancer, the general trend may reflectimprovements in the socioeconomic status o the population andperhaps some dietary changes. Te sudden increase in incidenceafer 1992, in the absence o a similar trend in mortality rates, mayreflect improvements in surveillance and early diagnosis techni-ques leading to earlier stages at diagnosis, when breast cancer ismore curable.
Te marked decline in incidence rates or cervical cancer since1962 most probably reflect the positive effects o screening andprevention programs based on vaginal cytology, as previouslydocumented, accompanied by a marked increase in the relativerequency o carcinoma in situ22. Mortality rates have also beendeclining since 1982.
Incidence rates or prostatic cancer show a marked increase since around 1982, not accompanied by a similar trend in mortality
rates. Tis most probably reflects early diagnosis via PSA testingTis phenomenon has also been observed in many other coun-tries. Tere is an ongoing discussion about the possible benefits ogeneralized PSA testing. Many early prostatic cancers may neverprogress to a threatening disease28, 29
Te increase in incidence rates o papillary carcinoma o thethyroid gland in women was noticed in an earlier publication22
No clear causal association is available. It seems to coincide withtrends or breast and colon carcinomas. Te observed decrease inincidence o ollicular carcinoma was predicted previously22andmay reflect the end o the epidemic o endemic goiter broughabout by iodine addition to table salt4.
During its 50 years o continuous operation the RPCC has hada clear impact on the national and the Latin American field ohealth services. It has ostered and guided the establishment oother Colombian population-based registries in the cities o PastoManizales, Bucaramanga and Barranquilla.
Te Registry has provided accurate and relevant inormation orthe education o health proessionals and supported communityefforts to design and establish programs or the prevention andcontrol o cancer. Internationally, it has contributed to all issueso the International Agency or Research on Cancer (IARC) oncancer statistics: Cancer Incidence in Five Continents and GLO-
BOCAN.
It inspired the creation and guided the operation o the Popula-tion-based Cancer Registry o Quito, Ecuador, now in continuouoperation or 19 years. Te new Latin American Registries will be
valuable in comparative studies o the incidence o specific typeso tumors in populations with considerable demographic and geographic diversity.
ACKNOWLEDGEMENTS:
Tis work was supported by grants o Universidad del Valle COLCIENCIAS 106-40820552. RC-302, 2007 (Colombia) andPPG CA 028842, National Cancer Institute, National Institutes oHealth (U.S.A.).
CONFLICT OF INTEREST DISCLOSURE:
Te authors declare that there is no real or potential conflict ointerest regarding the possible publication o this work.
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
8/11
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
9/11
253
Site
Age-Standardized (World) Mortality Rate by Period
1984-88 1989-93 1994-98 1999-03 2004-08
Male Female Male Female Male Female Male Female Male Female AP
Lip, oral cavity, pharynx 4.1 1.1 3.0 1.6 3.0 1.4 2.4 1.3 1.9 1.1 -3.6
Esophagus 3.9 1.7 3.4 1.8 3.6 1.5 2.7 1.3 2.0 0.8 -3.4
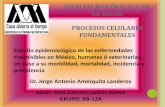
Stomach 26.8 15.9 25.9 14.6 22.0 12.9 19.9 10.7 18.2 9.8 -2.1
Colorectum 5.2 6.0 6.2 6.3 8.0 7.3 7.6 8.1 8.2 6.7 1.8
Liver 6.3 6.0 6.2 6.9 5.5 5.4 6.0 4.9 5.8 4.5 -0.4
Pancreas 4.1 4.9 5.6 4.2 4.6 4.4 4.7 4.1 3.7 3.2 -1.3
Larynx 3.2 1.2 3.2 0.8 2.2 0.9 2.5 0.6 2.2 0.3 -2.4
Bronchus, Lung 22.6 9.2 21.4 8.5 18.3 8.9 18.8 8.2 16.0 8.2 -1.7
Cervix Uteri 18.5 15.0 11.4 9.2 7.9
Corpus Uteri 2.2 3.4 3.2 2.9 1.7
Breast 11.9 14.7 14.0 16.2 13.7
Ovary 4.4 4.9 4.8 5.6 5.0
Prostate 15.4 16.6 19.7 18.6 17.5 0.3
Testis 0.4 0.5 0.3 0.4 0.3 ~
Bladder 3.0 2.0 2.3 0.9 2.1 1.1 2.8 0.8 1.9 0.8 -1.6
Thryroid 1.0 1.8 0.7 1.3 1.2 1.3 1.1 1.2 1.1 1.1 1.1
Lymphoma 6.0 4.8 7.5 4.7 6.7 5.0 6.3 4.3 5.5 4.5 -1.5
Leukaemia 4.7 3.9 5.6 4.6 6.1 4.9 5.4 4.1 5.5 4.5 0.2
Melanoma 1.3 1.1 1.4 1.0 1.8 1.3 2.0 1.3 2.2 1.2 2.0
All cancers excl. non-melanoma
skin cancer126.9 116.9 130.1 115.3 126.9 108.9 120.4 103.1 110.1 91.8 -0.8
Table 2.Cali, Colombia. Trends in Age-Standardized (World) Mortality Rates for Selected Sites by sex, through 1984-2008.
Rates are per 100,000 pers-years.
~ Statistic could not be calculated.
* The APC is significantly different from zero (p
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
10/11
254
REFERENCES
1. Correa P. Estudio estadistico del cancer en Antioquia. Antio-quia Med. 1955;5:589-605.2. Correa P. Statistical Study o cancer in Antioquia. Scweiz Z PathBakt. 1955;18:491-500.3. Correa P, Llanos G. Cancer incidence in Cali, Colombia. In:Doll R, Payne P, Waterhouse J, editors. Cancer Incidence in fiveContinents. Geneva: UICC Springer Verlag; 1966. p. 78-83.4. Gaitan E, Wahner HW, Correa P, Bernal R, Jubiz W, Gaitan JE.
Endemic goiter in the Cauca Valley. I. Results and limitations otwelve years o iodine prophylaxis. J Clin Endocrinol Metab. 1968;28(12):1730-40.5. Correa P, Llanos G. Morbidity and mortality rom cancer inCali, Colombia. J Nat Canc Inst. 1966;36(4):717.6. Aristizabal N, Cuello C, Correa P, Collazos , Haenszel W. Teimpact o vaginal cytology on cervical cancer risks in Cali, Colom-bia. Int J Cancer 1984;34(1):5-9.7. Correa P, Cuello C, Duque E. Carcinoma and intestinal meta-plasia o the stomach in Colombian migrants. J Natl Cancer Inst.1970;44(2):297-306.8. Parkin D, Chen V, Ferlay J, Galceran J, Storm HH, Whelan SL.Comparability and quality control in cancer registration. Lyon:
IARC, 1994.9. Curado M, Edwards B, Shin H, Storm H, Ferlay J, Heanue M.Cancer Incidence in Five Continents. Vol. IX. Lyon: IARC Press;2007.10. Doll R, Muir C, Waterhouse J. Cancer Incidence in Five Con-tinents. Vol II. New York: Springer-Verlag Berlin Heidelberg;1970.11. Muir C, Waterhouse J, Mack , Powell J, Whelan S. Cancer In-cidence in Five Continents. Vol. V. Lyon: IARC Press; 1987.12. Parkin D, Muir C, Whelan S, Gao Y, Ferlay J, Powell J. CancerIncidence in Five Continents. Vol. VI. Lyon: IARC Press; 1992.13. Parkin D, Whelan S, Ferlay J, Raymond L, Young J. CancerIncidence in Five Continents. Vol. VII. Lyon: IARC Press; 1997.
14. Parkin D, Whelan S, Ferlay J, eppo L, Tomas D. Cancer Inci-dence in Five Continents. Vol. VIII. Lyon: IARC Press; 2002.15. Waterhouse J, Muir C, Correa P, Powell J. Cancer Incidence inFive Continents. Vol. III.: IARC Press; 1976.16. Waterhouse J, Muir C, Shanmugaratnam K, Powell J. Cancer
Incidence in Five Continents. Vol. IV. Lyon: IARC Press; 1982.17. Ferlay J. IARCtools. 2 ed. Lyon, : IARC Press; 2000.18. Murray C, Lopez AD, Mathers CD, Stein C. Te Global Burden o Disease 2000 project: aims, methods and data sources. GPEDiscussion Paper No 36. Geneva: WHO; 2001.19. Estimaciones y proyecciones de poblacin periodo 1985-2020[database on the Internet]. DANE. [cited 2011]. Available romhttp://www.dane.gov.co.20. Boyle P, Parkin DM. Statistical methods or registries. In: O.M
Jensen DMP, R. MacLennan, C.S. Muir and R.G. Skee, editor. Cancer Registration: Principles and Methods. IARC Scientific Publi-cations. Lyon: IARC: IARC Scientific Publication No. 95; 1991. p126-58.21. Surveillance Research Program NCI. SEER*Stat sofware. 6.3.5ed. Bethesda, MD: National Cancer Institue; 2007.22. Cuello C, Correa P, Haenszel W. rends in cancer incidence inCali, Colombia. J Natl Cancer Inst. 1983 ;70(4):635-41.23. Murillo R, Pineros M, Hernandez G. Atlas de mortalidad porcancer en Colombia. Bogota: Instituto. Nacional de Cancerologa2003.24. HAENSZEL W. Cancer mortality among the oreign-born inthe United States. J Natl Cancer Inst. 1961;26:37-132.
25. Fox JG, Correa P, aylor NS, Zavala D, Fontham E, Janney FCampylobacter pylori-associated gastritis and immune responsein a population at increased risk o gastric carcinoma. Am J Gas-troenterol. 1989;84(7):775-81.26. Bosetti C, Malvezzi M, Chatenoud L, Negri E, Levi F, La Vec-chia C. rends in cancer mortality in the Americas, 1970-2000Ann Oncol. 2005;16(3):489-511.27. Menezes A, Lopez M, Hallal P, Muio A, Perez-Padilla R, Jardim J. Prevalence o smoking and incidence o initiation in theLatin American adult population: the PLAINO study. BMC PubHealth. 2009;9:151.28. Peres J. New PSA guidelines discourage overscreening. J NatCancer Inst. 2012;104(1):8-9.
29. Andriole GL, Craword ED, Grubb RL, Buys SS, Chia D, ChurchR. Prostate cancer screening in the randomized Prostate, LungColorectal, and Ovarian Cancer Screening rial: mortality resultsafer 13 years o ollow-up. J Natl Cancer Inst. 2012;104(2):125-32
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
-
8/12/2019 Cali Cncer 50 aos incidencia & mortalidad RPCC
11/11
255
Bravo LE et al / Colombia Mdica - Vol. 43 N 4, 2012 (Octubre-Diciembre)
Tendencia de la incidencia y mortalidad por cncer en Cali, Colombia. 50 aos de experiencia
RESUMEN
Propsito. El objetivo del Registro poblacional de cncer (RPCC) de Cali, es registrar todos los casos nuevos en residentes permanentes dentro de los lmites de Cali. Sedescriben las tendencias de la incidencia y mortalidad. El RPCC ha estado en operacin continua por 50 aos.Metodologa.Los casos registrados son obtenidos mediante bsqueda activa en las uentes de inormacin como: hospitales, laboratorios de Patologa y Hematologa
centros de Radioterapia, oficina estatales en las que se procesan los certificados de deuncin y consultorios de mdicos privados. Se estima que el proceso de registro ecompleto en un 95%.Resultados. Se describe una disminucin drstica en la incidencia de tumores relacionados con agentes inecciosos, especialmente los casos de cncer de cuello uterinoy estmago. Se documenta incremento gradual en las tasas de incidencia de los tumores asociados con la afluencia y el sndrome metablico, especialmente el cncer dcolon y mama en la mujer. Se advierte un aumento inesperado de la incidencia de carcinoma papilar en la glndula tiroides en mujeres. Los tipos de cncer relacionadocon el consumo de tabaco, especialmente el de pulmn, mostraron un aumento de la incidencia alrededor de 1970, aparentemente el comienzo de una epidemia similar ala reportada en sociedades occidentales. Pero el incremento de la incidencia se detuvo en 1980, resultado de una uerte campaa anti-tabaco liderada en Colombia en losetenta.Conclusiones.Los resultados han influido en las estrategias de prevencin aplicadas por las autoridades de salud pblica, en especial el establecimiento de un programapara toda la ciudad para prevenir el cncer de cuello uterino a travs del uso generalizado de la citologa vaginal y las campaas contra el tabaquismo. Adems, se hanestablecido nuevos registros poblacionales de cncer en otras ciudades de Colombia y en Ecuador.
Palabras claves: Cncer; Epidemiologa; Cali; Colombia; endencias del cncer
Bravo LE, Collazos T, Collazos P, Garca LS, Correa P.Trends of cancer incidence and mortality in Cali, Colombia 50 years experience.Colomb. Med. 2012; 43(4) 246-255