BASES BIOLÓGICAS DEL CÁNCER DE...
30
BASES BIOLÓGICAS DEL CÁNCER DE PRÓSTATA Rebeca Lozano Mejorada Unidad de Investigación Clínica en Cáncer de Próstata, CNIO Unidad de Investigación Tumores Genitourinarios, CNIO-IBIMA
Transcript of BASES BIOLÓGICAS DEL CÁNCER DE...
BASES BIOLÓGICAS DEL CÁNCER DE PRÓSTATA
Rebeca Lozano Mejorada
Unidad de Investigación Clínica en Cáncer de Próstata, CNIO
Unidad de Investigación Tumores Genitourinarios, CNIO-IBIMA
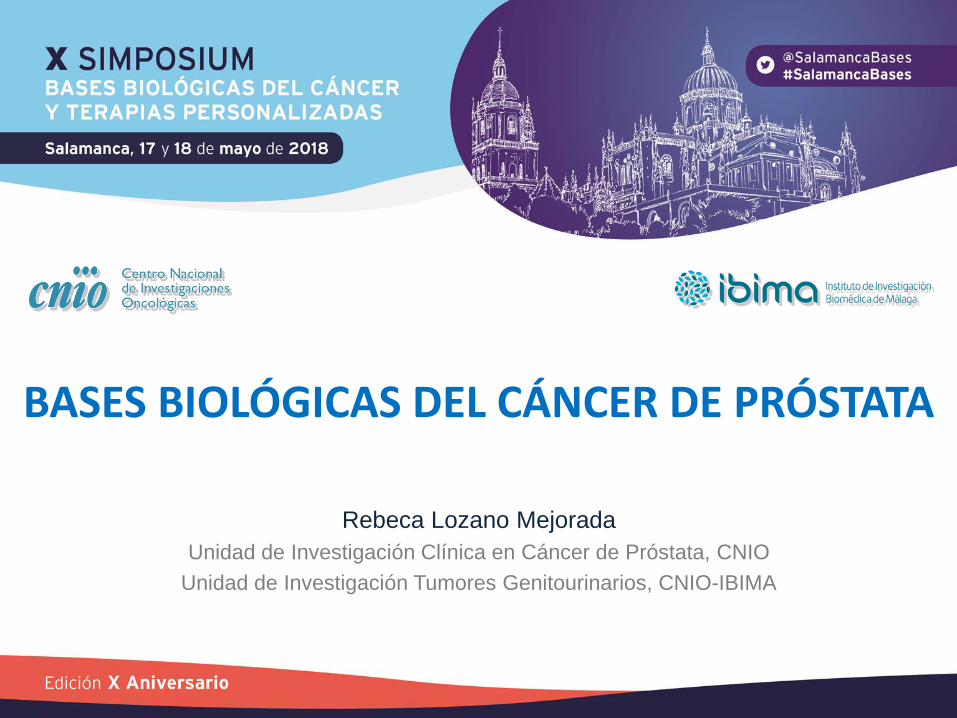
TIMELINE PROSTATE CANCER
1940s 1996
ADT
2004 2010 2011 2012 2013 2014 2017 2018
Docetaxel TAX327
SWOG 9916
Mitoxantrone CALGB 9182
Sipuleucel T IMPACT
Cabazitaxel TROPIC
Abiraterone COU-AA-301
Enzalutamide AFFIRM
Abiraterone COU-AA-302
Enzalutamide PREVAIL
Radium-223 ALSYMPCA
Enzalutamide PROSPER
Apalutamide SPARTAN
Docetaxel CHAARTED STAMPEDE
Abiraterone LATITUDE
STAMPEDE
2015 2016
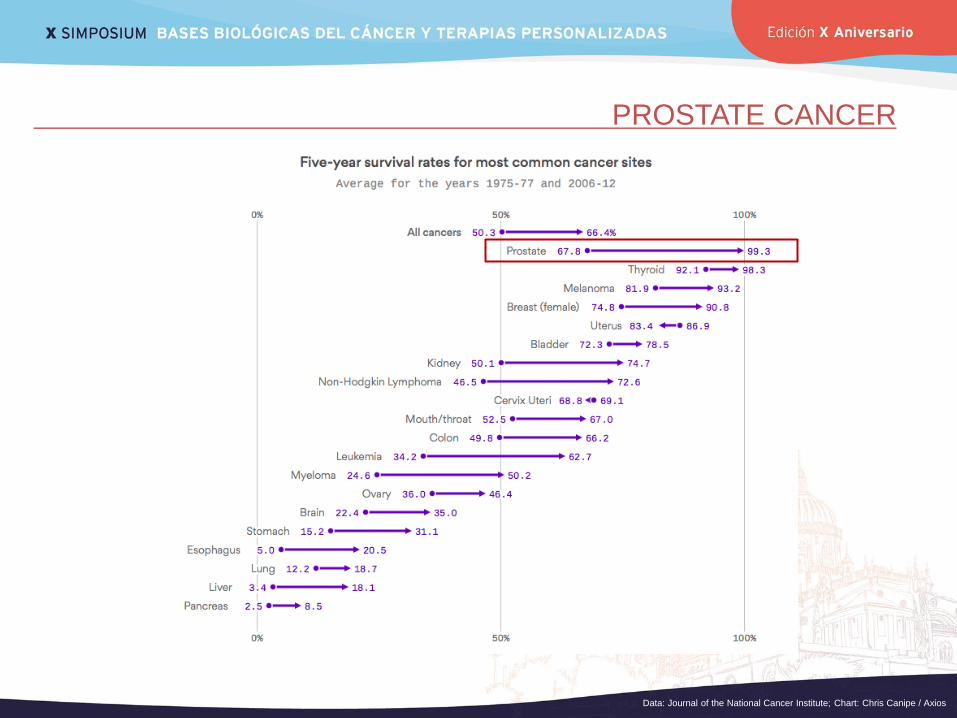
PROSTATE CANCER
Data: Journal of the National Cancer Institute; Chart: Chris Canipe / Axios
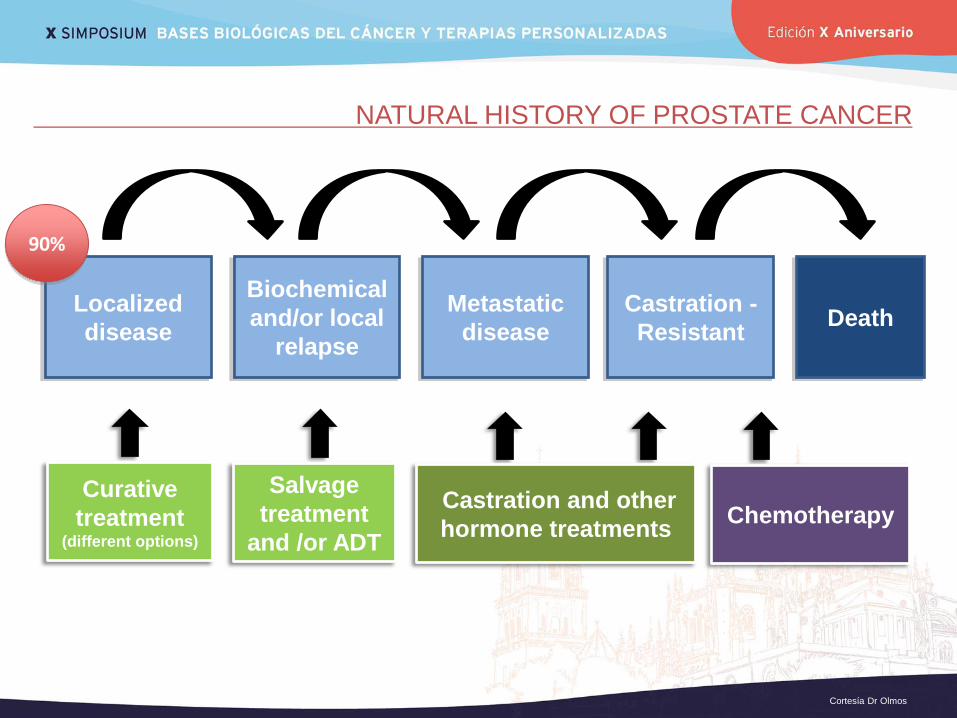
Localized
disease
Biochemical
and/or local
relapse
Metastatic
disease
Castration -
Resistant Death
90%
Curative
treatment (different options)
Salvage
treatment
and /or ADT
Castration and other
hormone treatments Chemotherapy
NATURAL HISTORY OF PROSTATE CANCER
Cortesía Dr Olmos
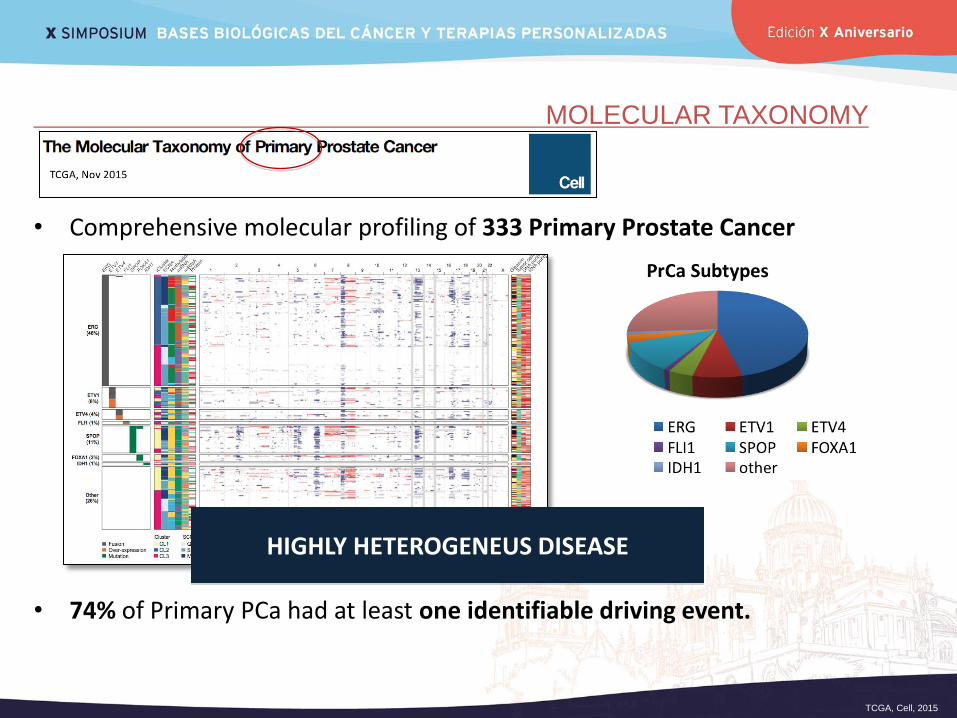
MOLECULAR TAXONOMY
• Comprehensive molecular profiling of 333 Primary Prostate Cancer
• 74% of Primary PCa had at least one identifiable driving event.
TCGA, Cell, 2015
HIGHLY HETEROGENEUS DISEASE
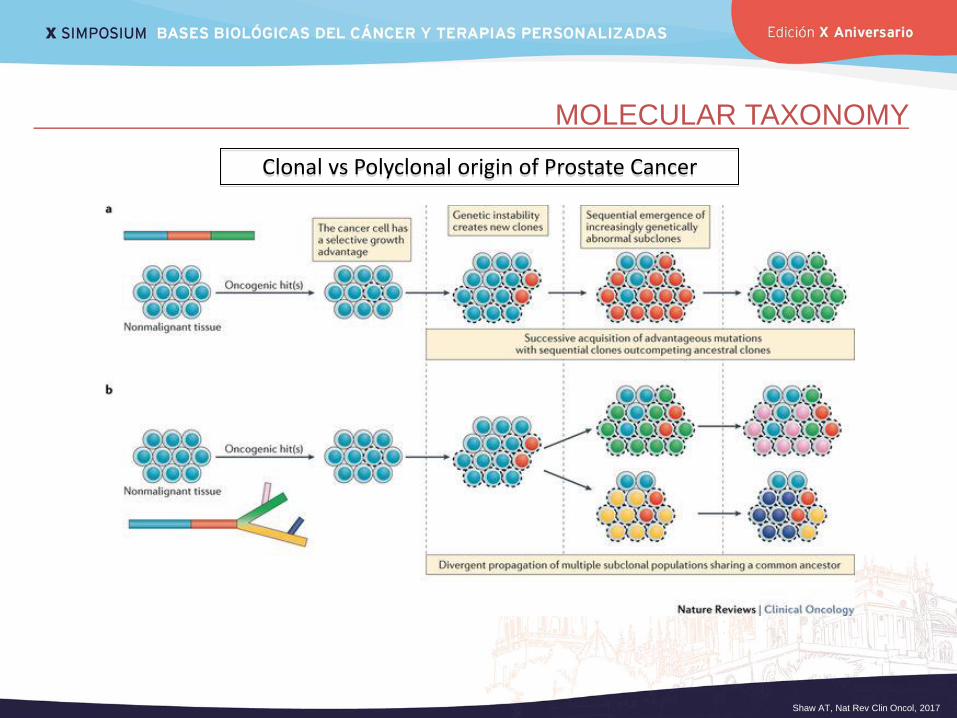
MOLECULAR TAXONOMY
Shaw AT, Nat Rev Clin Oncol, 2017
Clonal vs Polyclonal origin of Prostate Cancer
MOLECULAR TAXONOMY
Espiritu SMG, Cell, 2018
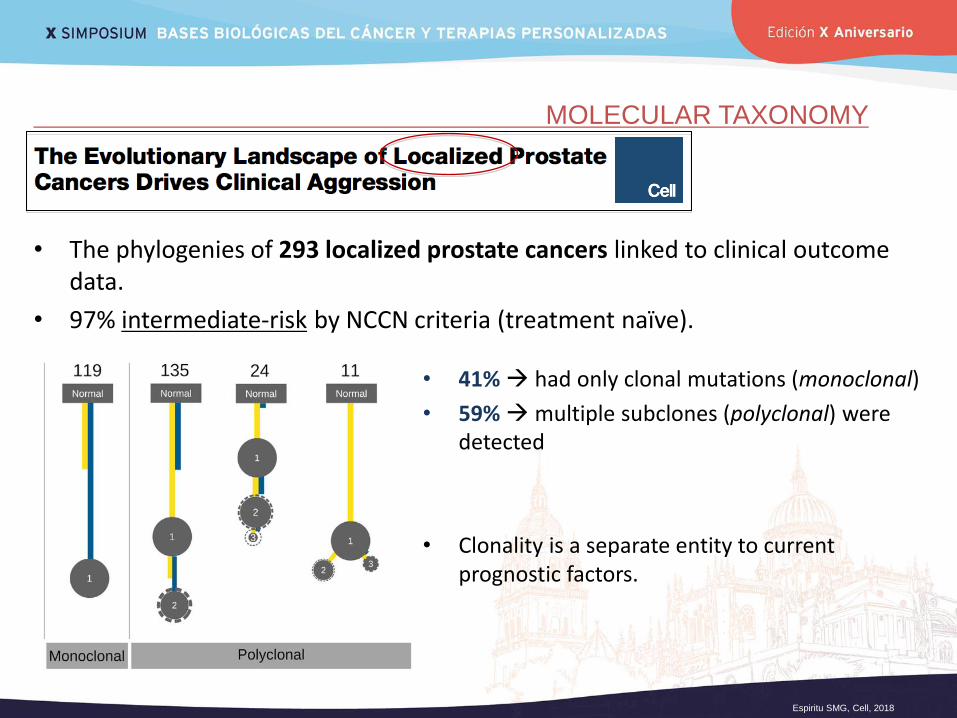
• The phylogenies of 293 localized prostate cancers linked to clinical outcome data.
• 97% intermediate-risk by NCCN criteria (treatment naïve).
• 41% had only clonal mutations (monoclonal)
• 59% multiple subclones (polyclonal) were detected
• Clonality is a separate entity to current prognostic factors.
MOLECULAR TAXONOMY
Espiritu SMG, Cell, 2018
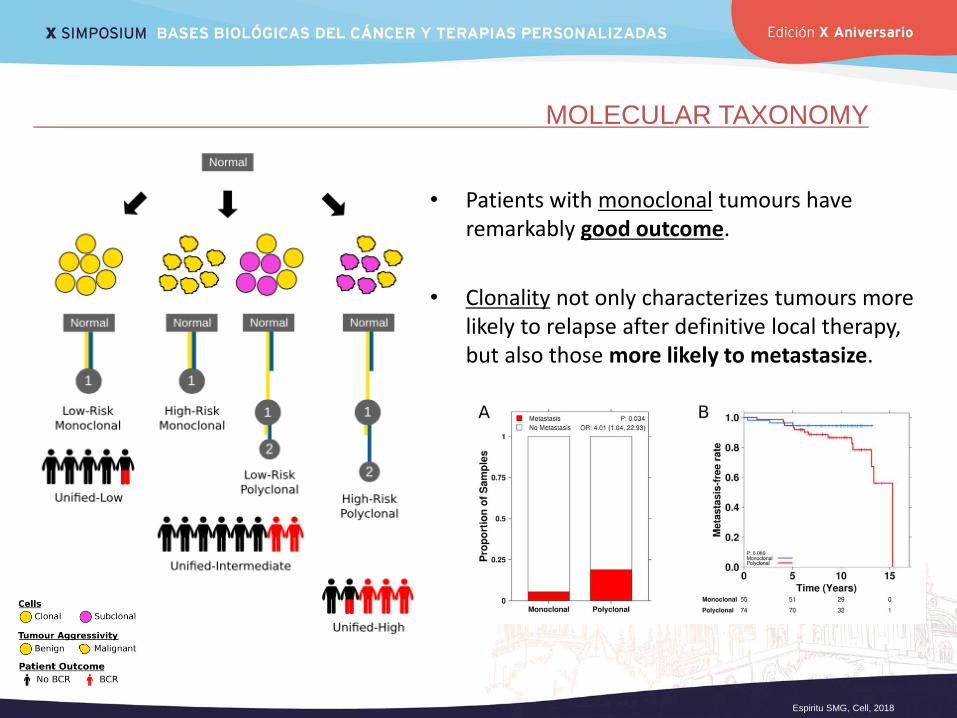
• Patients with monoclonal tumours have remarkably good outcome.
• Clonality not only characterizes tumours more likely to relapse after definitive local therapy, but also those more likely to metastasize.
MOLECULAR TAXONOMY
Robinson D, Cell, 2015
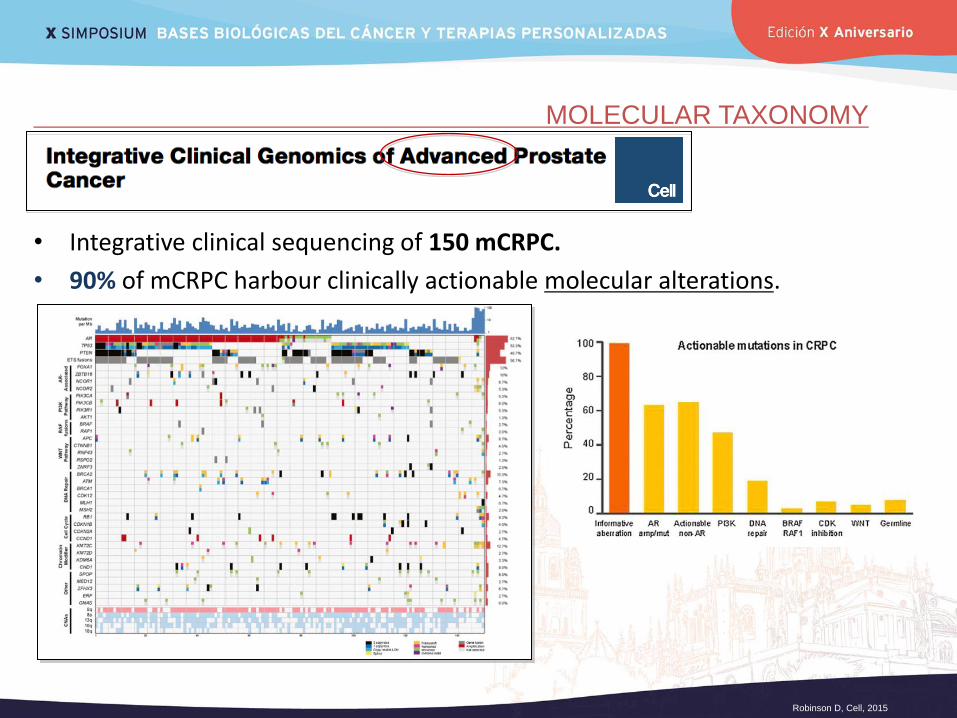
• Integrative clinical sequencing of 150 mCRPC.
• 90% of mCRPC harbour clinically actionable molecular alterations.
MOLECULAR TAXONOMY
Armenia J, Nature Genetics, 2018
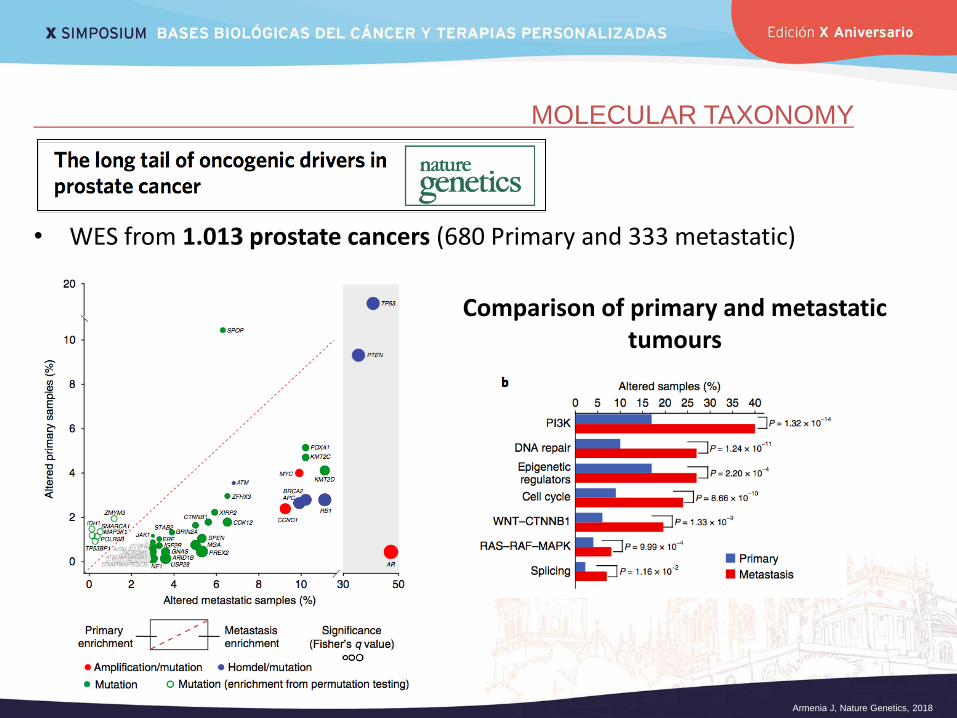
Comparison of primary and metastatic tumours
• WES from 1.013 prostate cancers (680 Primary and 333 metastatic)
MOLECULAR TAXONOMY
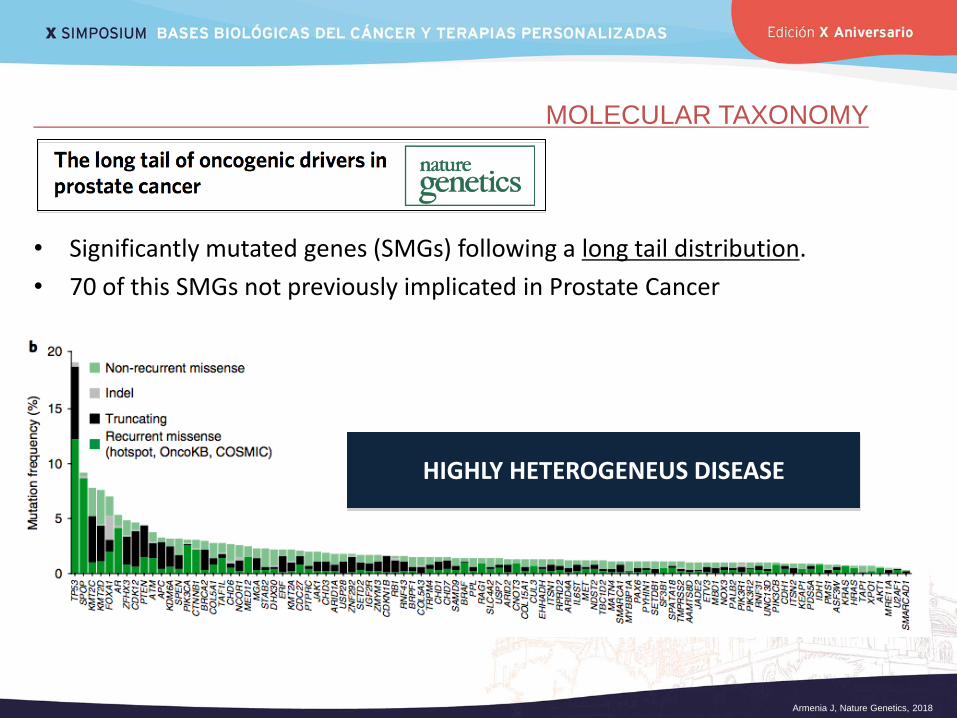
Armenia J, Nature Genetics, 2018
• Significantly mutated genes (SMGs) following a long tail distribution.
• 70 of this SMGs not previously implicated in Prostate Cancer
HIGHLY HETEROGENEUS DISEASE
PROSTATE SPECIFIC MEMBRANE ANTIGEN (PSMA)
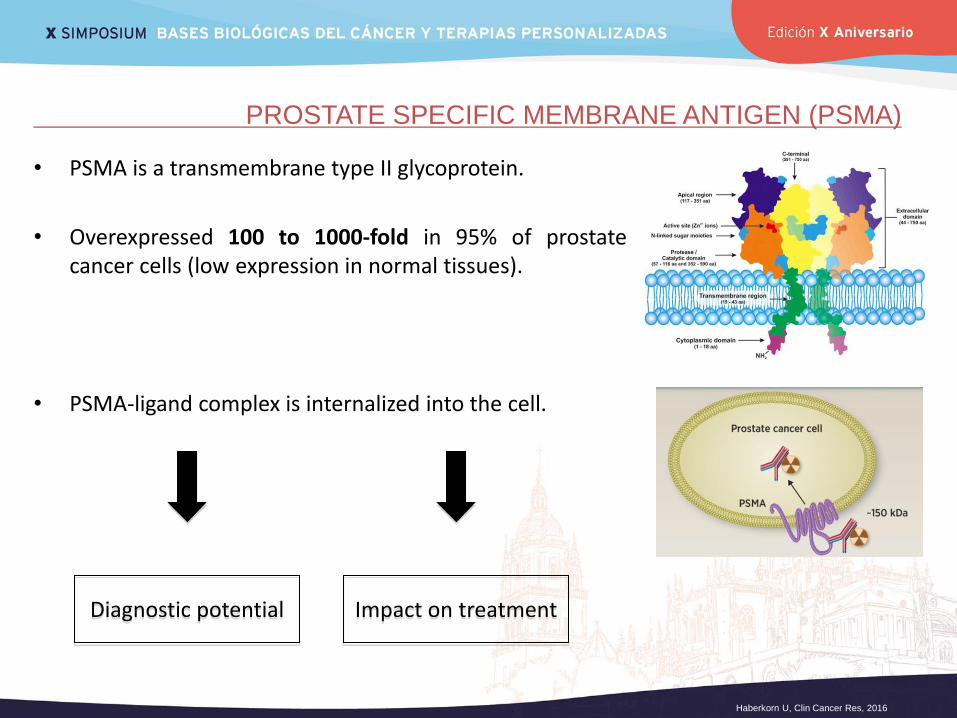
• PSMA is a transmembrane type II glycoprotein.
• Overexpressed 100 to 1000-fold in 95% of prostate cancer cells (low expression in normal tissues).
• PSMA-ligand complex is internalized into the cell.
Diagnostic potential Impact on treatment
Haberkorn U, Clin Cancer Res, 2016
PROSTATE SPECIFIC MEMBRANE ANTIGEN (PSMA)
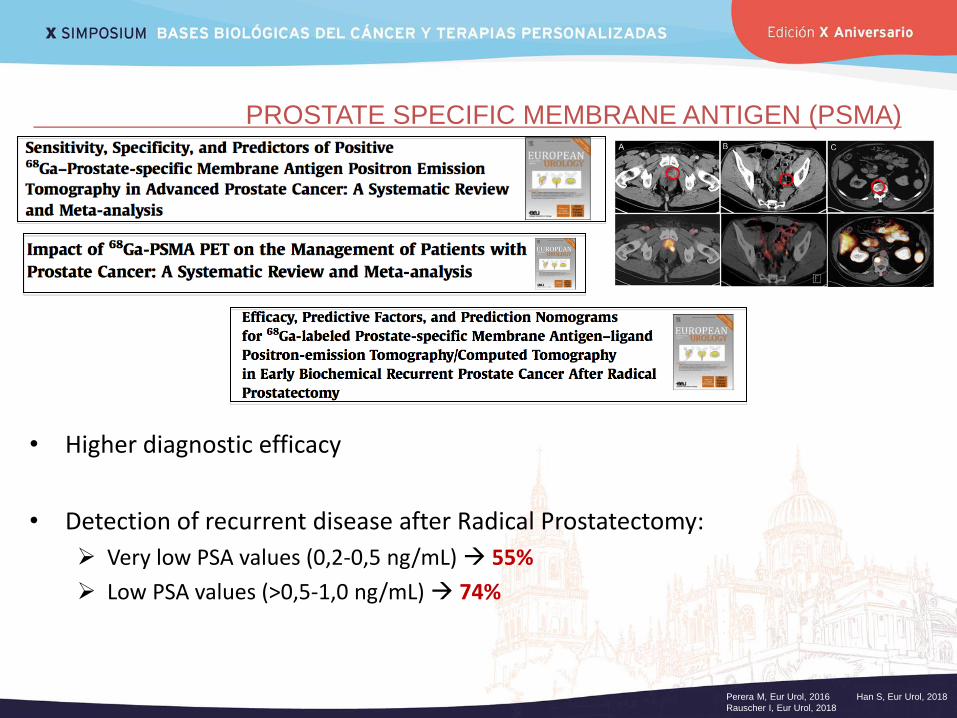
• Higher diagnostic efficacy
• Detection of recurrent disease after Radical Prostatectomy:
Very low PSA values (0,2-0,5 ng/mL) 55%
Low PSA values (>0,5-1,0 ng/mL) 74%
Perera M, Eur Urol, 2016 Han S, Eur Urol, 2018
Rauscher I, Eur Urol, 2018
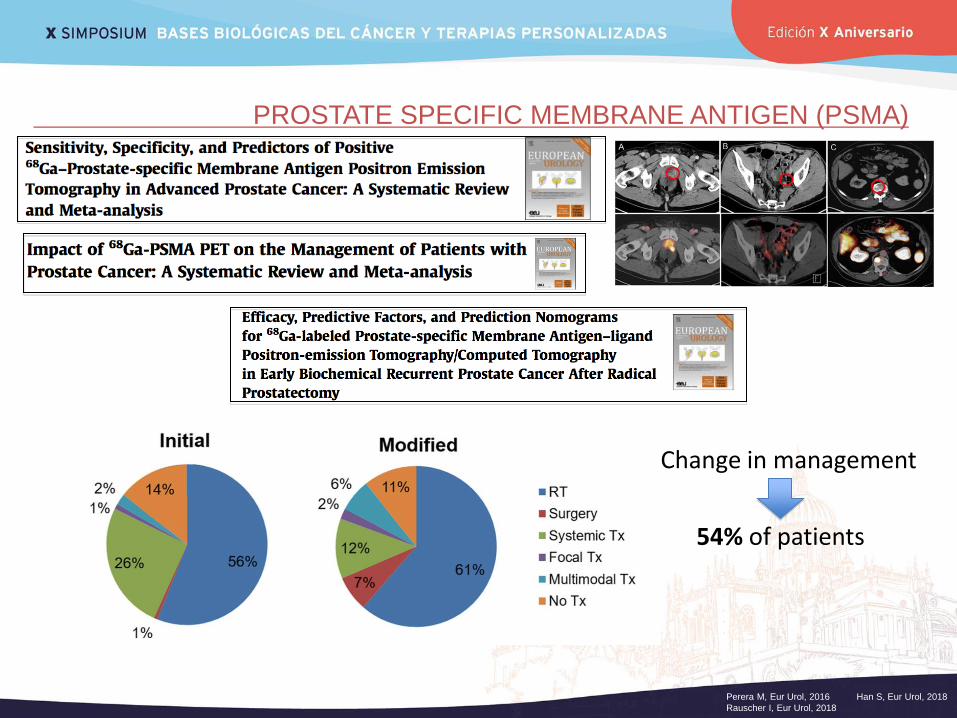
PROSTATE SPECIFIC MEMBRANE ANTIGEN (PSMA)
Change in management
54% of patients
Perera M, Eur Urol, 2016 Han S, Eur Urol, 2018
Rauscher I, Eur Urol, 2018
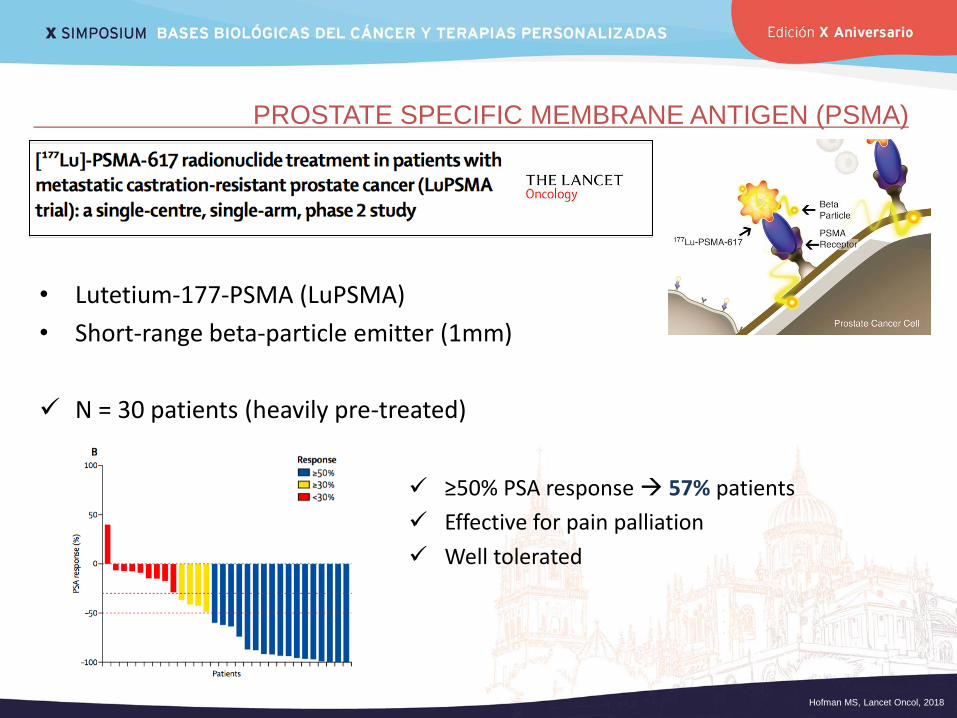
PROSTATE SPECIFIC MEMBRANE ANTIGEN (PSMA)
• Lutetium-177-PSMA (LuPSMA)
• Short-range beta-particle emitter (1mm)
N = 30 patients (heavily pre-treated)
≥50% PSA response 57% patients
Effective for pain palliation
Well tolerated
Hofman MS, Lancet Oncol, 2018
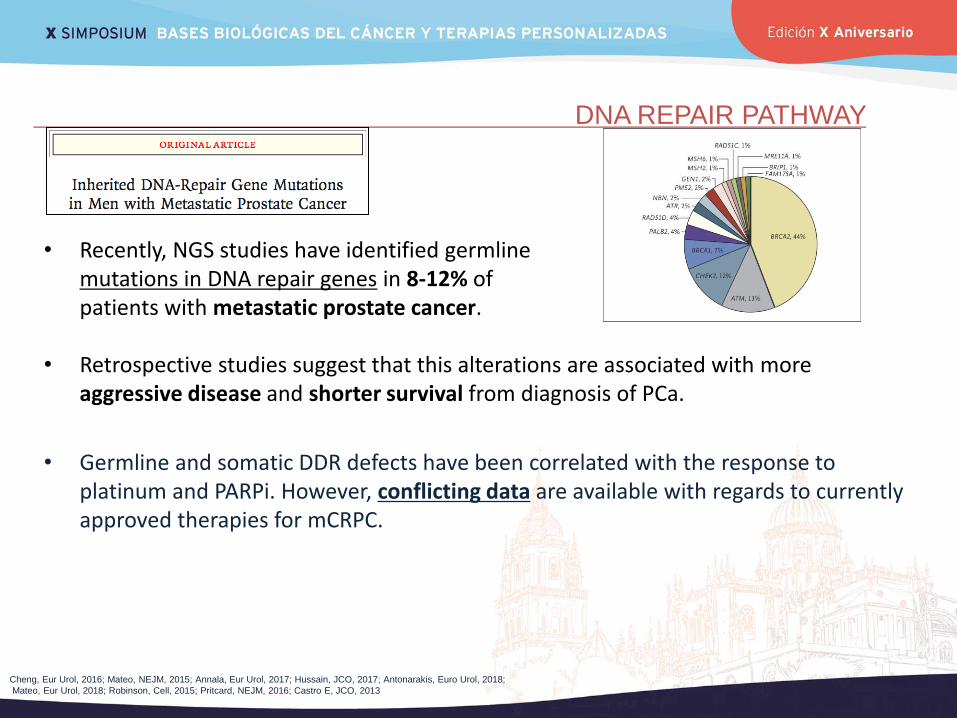
• Retrospective studies suggest that this alterations are associated with more aggressive disease and shorter survival from diagnosis of PCa.
• Germline and somatic DDR defects have been correlated with the response to platinum and PARPi. However, conflicting data are available with regards to currently approved therapies for mCRPC.
DNA REPAIR PATHWAY
Cheng, Eur Urol, 2016; Mateo, NEJM, 2015; Annala, Eur Urol, 2017; Hussain, JCO, 2017; Antonarakis, Euro Urol, 2018;
Mateo, Eur Urol, 2018; Robinson, Cell, 2015; Pritcard, NEJM, 2016; Castro E, JCO, 2013
• Recently, NGS studies have identified germline mutations in DNA repair genes in 8-12% of patients with metastatic prostate cancer.
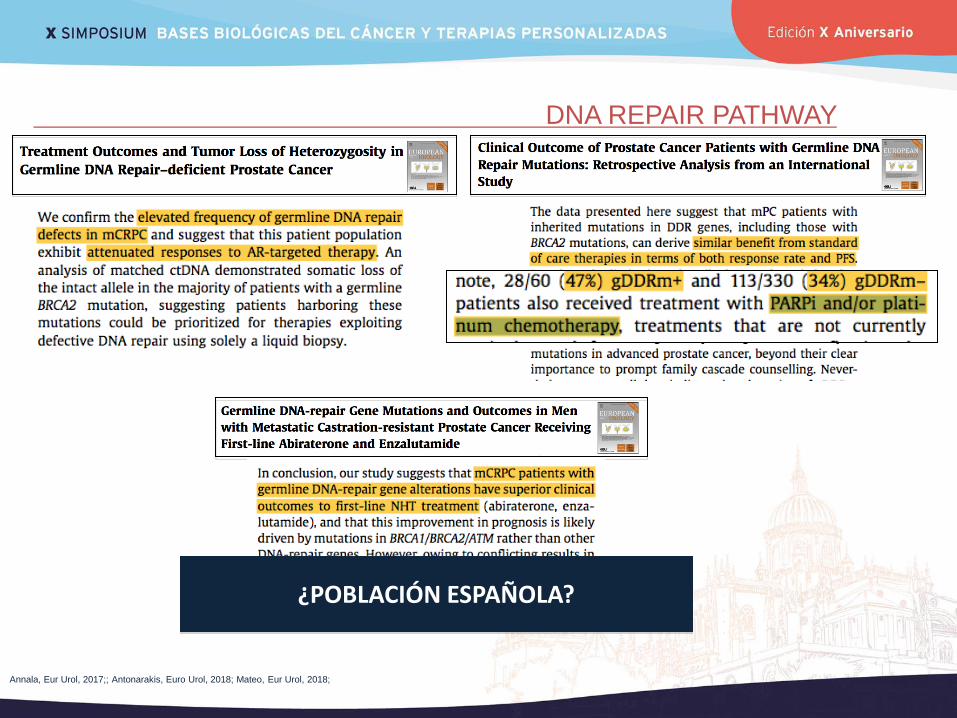
DNA REPAIR PATHWAY
Annala, Eur Urol, 2017;; Antonarakis, Euro Urol, 2018; Mateo, Eur Urol, 2018;
¿POBLACIÓN ESPAÑOLA?
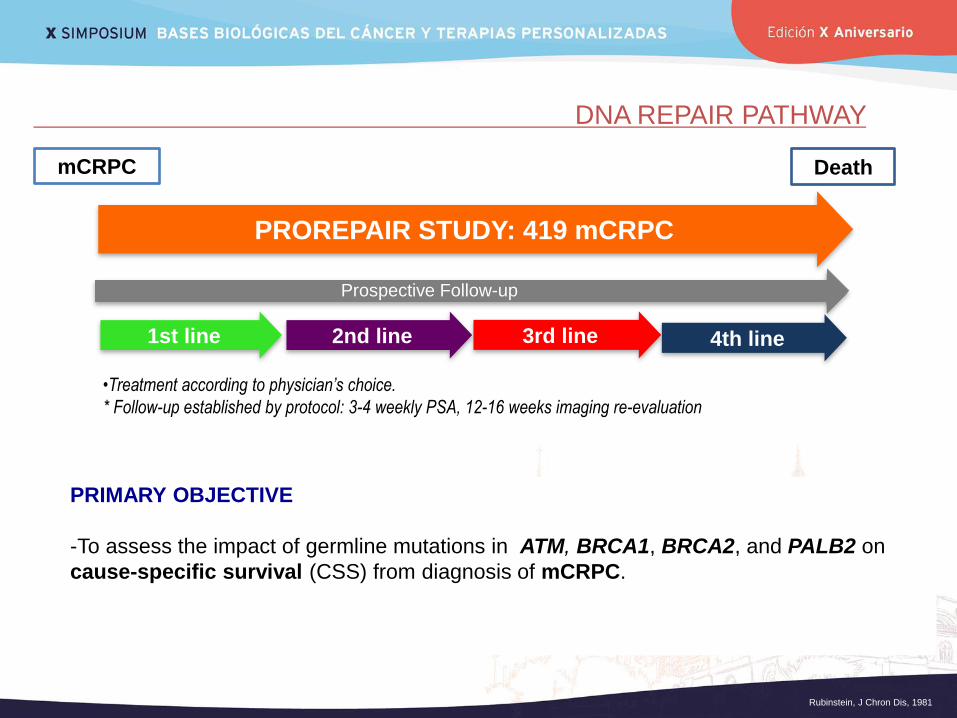
DNA REPAIR PATHWAY
PROREPAIR STUDY: 419 mCRPC
1st line 2nd line 3rd line
mCRPC
Prospective Follow-up
Death
4th line
•Treatment according to physician’s choice.
* Follow-up established by protocol: 3-4 weekly PSA, 12-16 weeks imaging re-evaluation
Rubinstein, J Chron Dis, 1981
PRIMARY OBJECTIVE
-To assess the impact of germline mutations in ATM, BRCA1, BRCA2, and PALB2 on
cause-specific survival (CSS) from diagnosis of mCRPC.
DNA REPAIR PATHWAY
Castro E, ESMO 2017
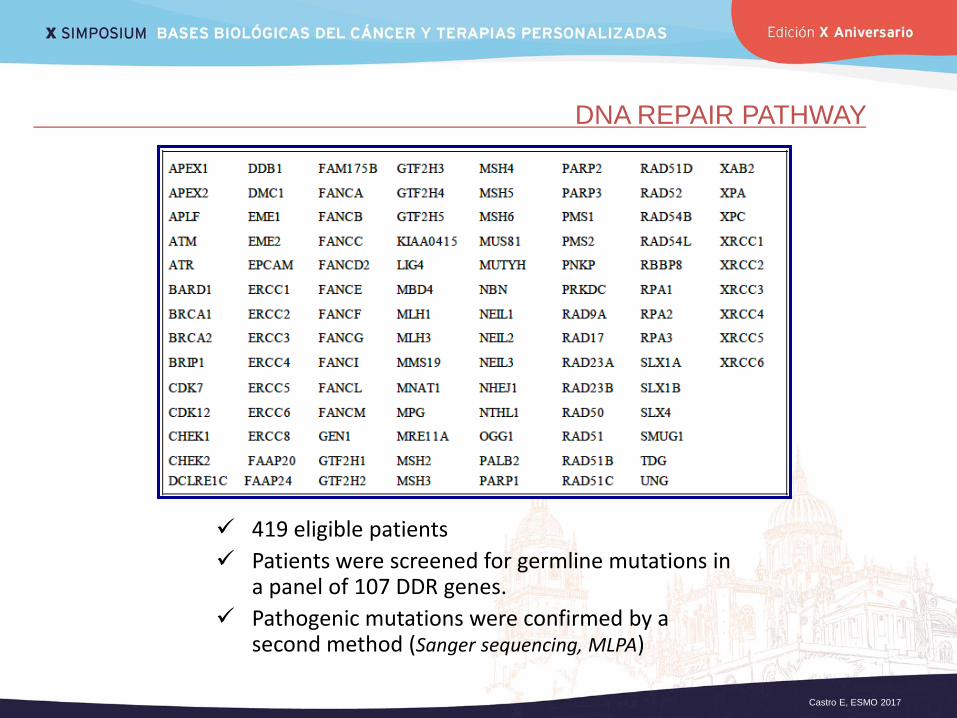
419 eligible patients
Patients were screened for germline mutations in a panel of 107 DDR genes.
Pathogenic mutations were confirmed by a second method (Sanger sequencing, MLPA)
DNA REPAIR PATHWAY
Castro E, ESMO 2017
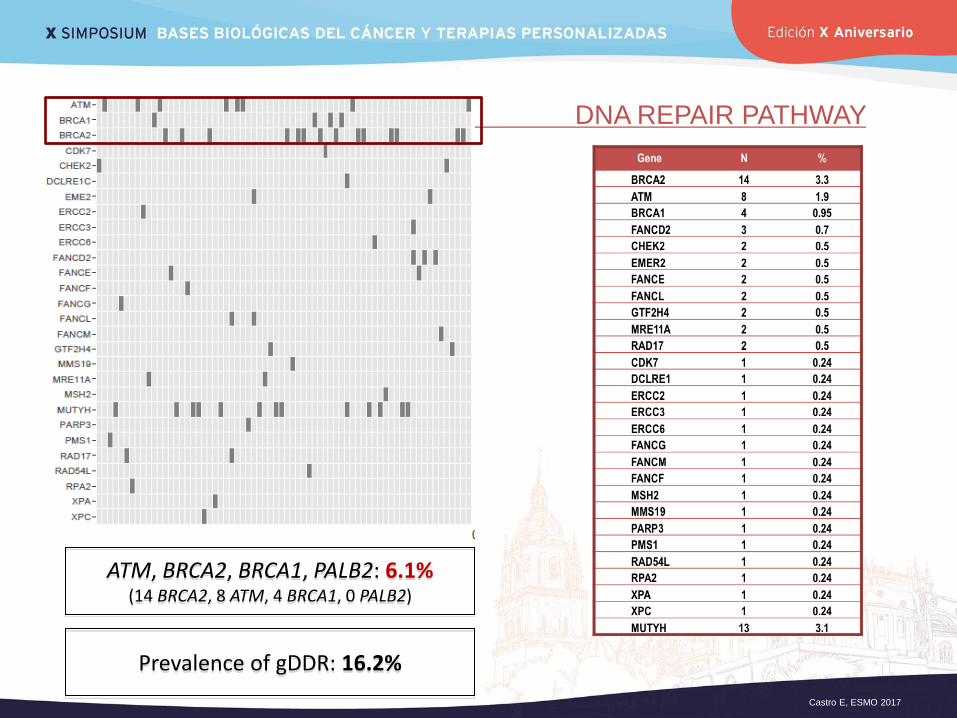
ATM, BRCA2, BRCA1, PALB2: 6.1% (14 BRCA2, 8 ATM, 4 BRCA1, 0 PALB2)
Prevalence of gDDR: 16.2%
DNA REPAIR PATHWAY
Non Carriers gDDR+ P Value
(gDDR+ vs Non-
Carriers)
ATM, BRCA1,
BRCA2
P value
(ATM,BRCA1/2, vs
No ATM,BRCA1/2)
BRCA2
carriers
P value (BRCA2 vs No
BRCA2)
Age at mCRPC (yrs)
- Median (range)
71.8
(46.6-93.8)
69.3
(50.7-86.6)
0.11
67.1
(52.1-86.6)
0.31
68.9
(52.1-77.6) 0.20
PSA at mCRPC (ng/dl)
- Median (range)
27.5
(0.03-1980)
24.81
(0.93.756)
0.806
29.4
(2.20-580)
0.61
51.6
(2.20-580)
0.30
Progression to mCRPC
• Only PSA
• Radiological
220 (62.7%)
131 (37.3%)
36 (52.9%)
32 (47.1%)
0.13
10 (38.5%)
16 (61.5%)
0.02
4 (28.6%)
10 (71.4%)
0.01
Metastasis sites
• Nodal
• Bone
• Visceral
166 (47.3%)
289 (82.3%)
32 (9.1%)
31 (45.6%)
60 (88.2%)
10 (14.7%)
0.90
0.29
0.18
15 (57.7%)
24 (92.3%)
3 (11.5%)
0.31
0.20
0.74
9 (64.3%)
13 (92.9%)
3 (21.4%)
0.27
0.33
0.16
Performance Status
• ECOG 0
• ECOG 1
• ECOG 2
1178 (50.7%)
144 (41%)
29 (8.3%)
25 (36.8%)
40 (58.8%)
3 (4.4%)
0.225
8 (30.8%)
15 (57.7%)
3 (11.5%)
0.07
5 (28.6%)
7 (50%)
2 (14.3%)
0.24
Elevated ALP (>ULN) 150 (42.7%) 29 (42.6%) 1.0 13 (50%) 0.54 9 (64.3%) 0.11
Elevated LDH (>ULN) 114 (32.9%) 23 (34.3%) 0.89 10 (40%) 0.51 6 (42.9%) 0.56
Haemoglobin <10 g/dl 18 (5.1%) 2 (2.9%) 0.75 2 (7.7%) 0.36 2 (14.3%) 0.14
Albumin <3.5 g/dl 23 (6.6%) 4 (6.1%) 1.0 1 (3.8%) 0.56 1 (7.1%) 0.93
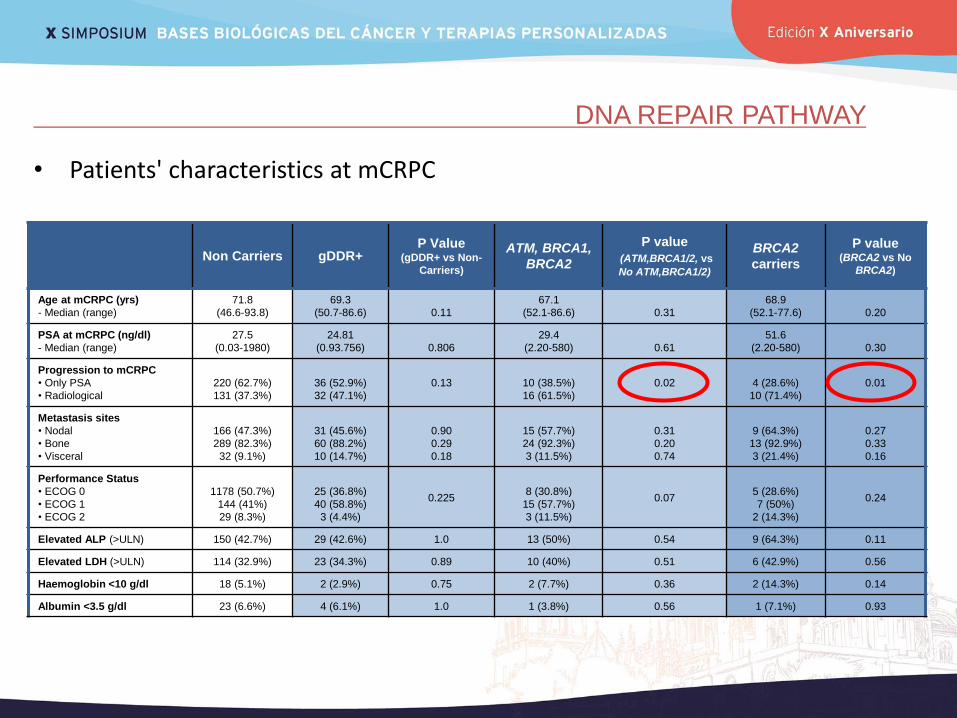
• Patients' characteristics at mCRPC
DNA REPAIR PATHWAY
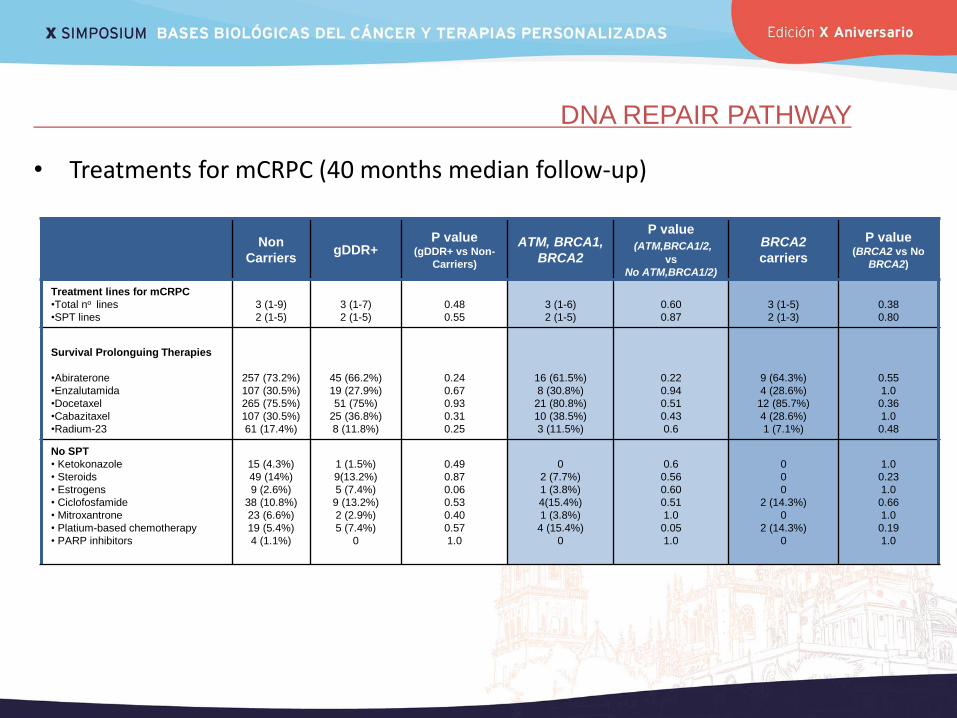
• Treatments for mCRPC (40 months median follow-up)
Non
Carriers gDDR+
P value (gDDR+ vs Non-
Carriers)
ATM, BRCA1,
BRCA2
P value
(ATM,BRCA1/2,
vs
No ATM,BRCA1/2)
BRCA2
carriers
P value (BRCA2 vs No
BRCA2)
Treatment lines for mCRPC
•Total no lines
•SPT lines
3 (1-9)
2 (1-5)
3 (1-7)
2 (1-5)
0.48
0.55
3 (1-6)
2 (1-5)
0.60
0.87
3 (1-5)
2 (1-3)
0.38
0.80
Survival Prolonguing Therapies
•Abiraterone
•Enzalutamida
•Docetaxel
•Cabazitaxel
•Radium-23
257 (73.2%)
107 (30.5%)
265 (75.5%)
107 (30.5%)
61 (17.4%)
45 (66.2%)
19 (27.9%)
51 (75%)
25 (36.8%)
8 (11.8%)
0.24
0.67
0.93
0.31
0.25
16 (61.5%)
8 (30.8%)
21 (80.8%)
10 (38.5%)
3 (11.5%)
0.22
0.94
0.51
0.43
0.6
9 (64.3%)
4 (28.6%)
12 (85.7%)
4 (28.6%)
1 (7.1%)
0.55
1.0
0.36
1.0
0.48
No SPT
• Ketokonazole
• Steroids
• Estrogens
• Ciclofosfamide
• Mitroxantrone
• Platium-based chemotherapy
• PARP inhibitors
15 (4.3%)
49 (14%)
9 (2.6%)
38 (10.8%)
23 (6.6%)
19 (5.4%)
4 (1.1%)
1 (1.5%)
9(13.2%)
5 (7.4%)
9 (13.2%)
2 (2.9%)
5 (7.4%)
0
0.49
0.87
0.06
0.53
0.40
0.57
1.0
0
2 (7.7%)
1 (3.8%)
4(15.4%)
1 (3.8%)
4 (15.4%)
0
0.6
0.56
0.60
0.51
1.0
0.05
1.0
0
0
0
2 (14.3%)
0
2 (14.3%)
0
1.0
0.23
1.0
0.66
1.0
0.19
1.0
DNA REPAIR PATHWAY
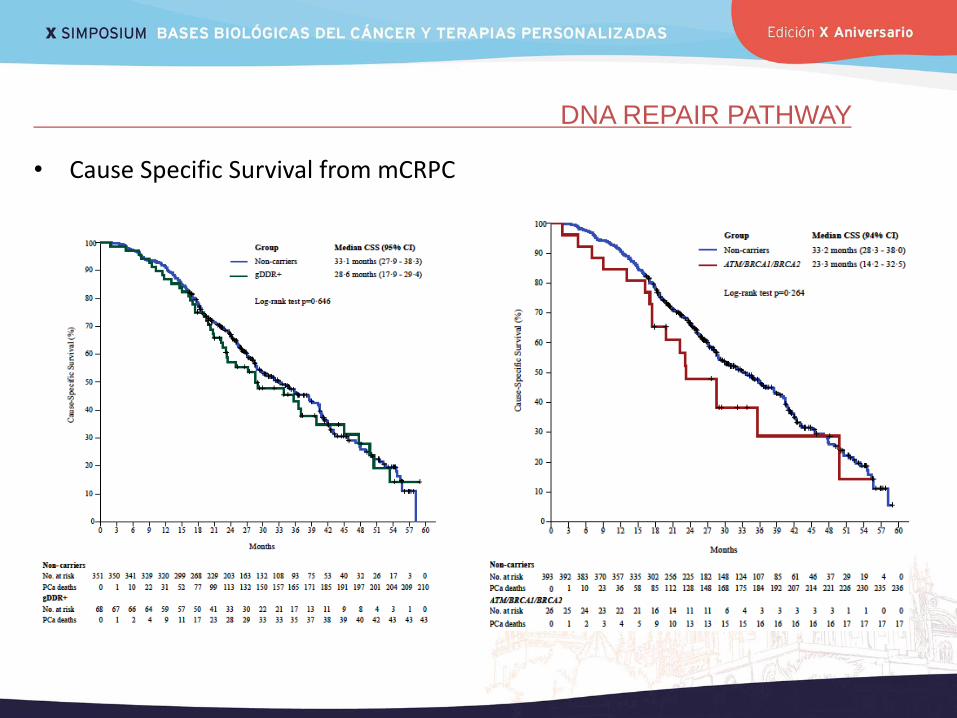
• Cause Specific Survival from mCRPC
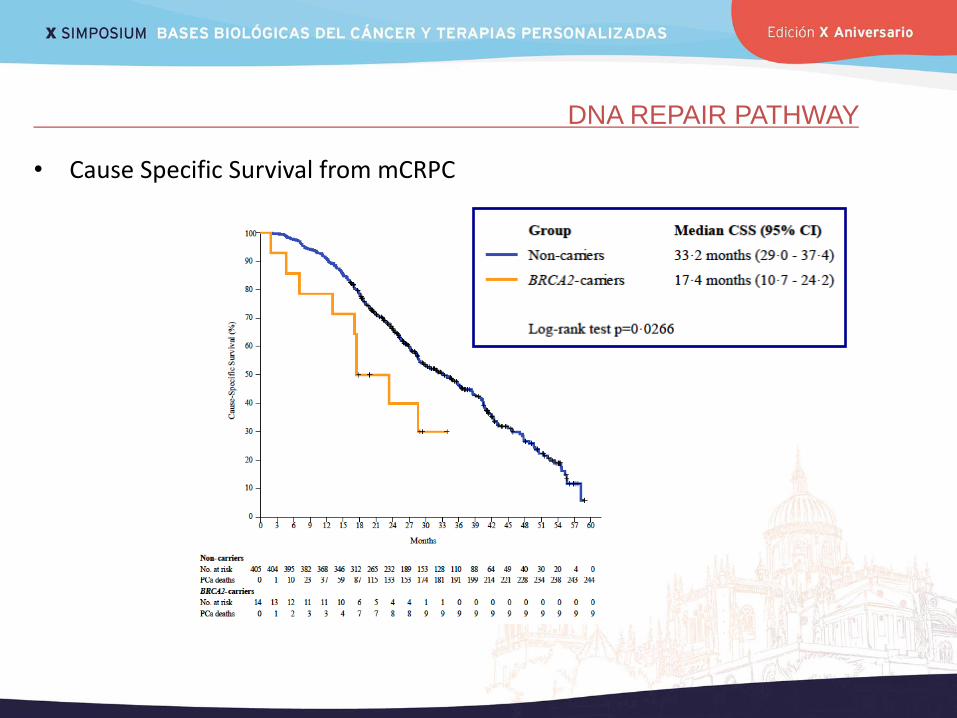
DNA REPAIR PATHWAY
• Cause Specific Survival from mCRPC
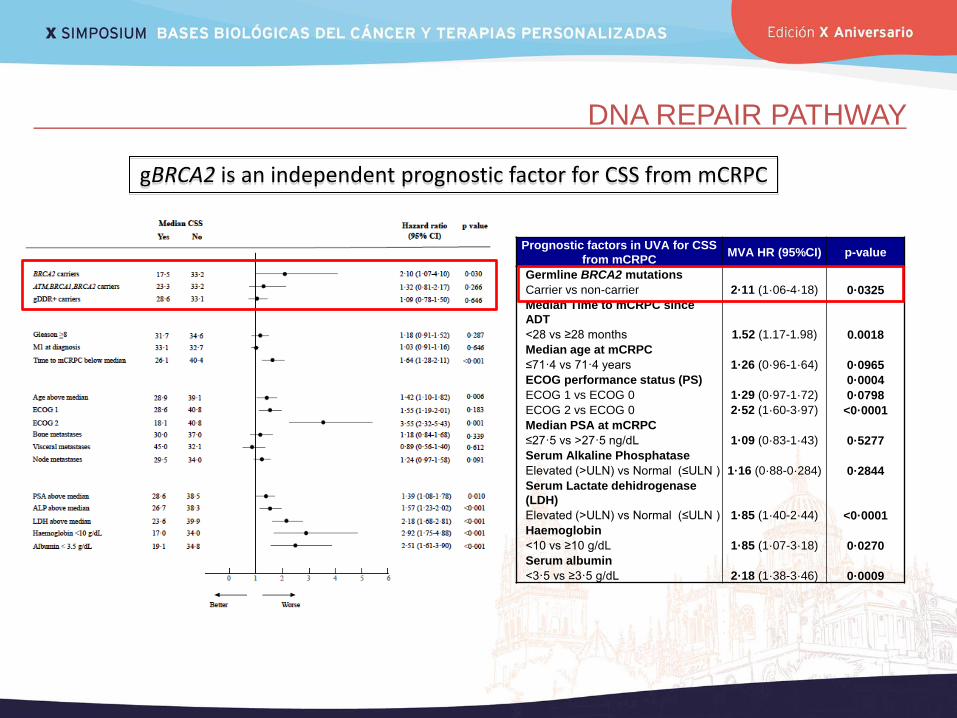
DNA REPAIR PATHWAY
Prognostic factors in UVA for CSS
from mCRPC MVA HR (95%CI) p-value
Germline BRCA2 mutations
0·0325 Carrier vs non-carrier 2·11 (1·06-4·18)
Median Time to mCRPC since
ADT
0.0018 <28 vs ≥28 months 1.52 (1.17-1.98)
Median age at mCRPC
0·0965 ≤71·4 vs 71·4 years 1·26 (0·96-1·64)
ECOG performance status (PS) 0·0004
ECOG 1 vs ECOG 0 1·29 (0·97-1·72) 0·0798
ECOG 2 vs ECOG 0 2·52 (1·60-3·97) <0·0001
Median PSA at mCRPC
0·5277 ≤27·5 vs >27·5 ng/dL 1·09 (0·83-1·43)
Serum Alkaline Phosphatase
0·2844 Elevated (>ULN) vs Normal (≤ULN ) 1·16 (0·88-0·284)
Serum Lactate dehidrogenase
(LDH)
<0·0001 Elevated (>ULN) vs Normal (≤ULN ) 1·85 (1·40-2·44)
Haemoglobin
0·0270 <10 vs ≥10 g/dL 1·85 (1·07-3·18)
Serum albumin
0·0009 <3·5 vs ≥3·5 g/dL 2·18 (1·38-3·46)
gBRCA2 is an independent prognostic factor for CSS from mCRPC
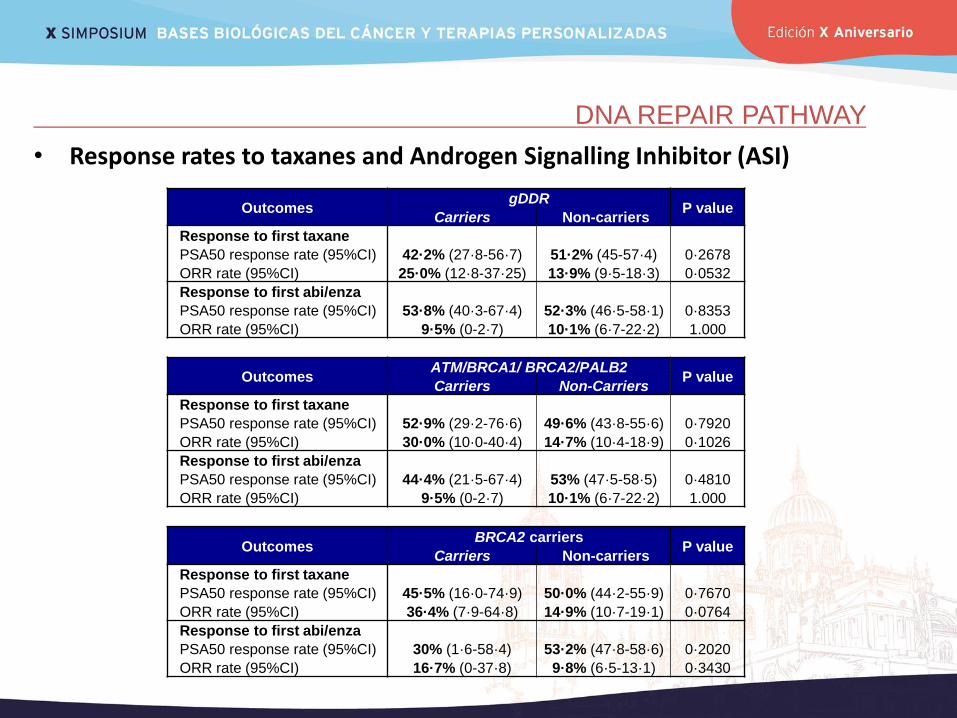
DNA REPAIR PATHWAY
• Response rates to taxanes and Androgen Signalling Inhibitor (ASI)
Outcomes gDDR
P value Carriers Non-carriers
Response to first taxane
PSA50 response rate (95%CI) 42·2% (27·8-56·7) 51·2% (45-57·4) 0·2678
ORR rate (95%CI) 25·0% (12·8-37·25) 13·9% (9·5-18·3) 0·0532
Response to first abi/enza
PSA50 response rate (95%CI) 53·8% (40·3-67·4) 52·3% (46·5-58·1) 0·8353
ORR rate (95%CI) 9·5% (0-2·7) 10·1% (6·7-22·2) 1.000
Outcomes ATM/BRCA1/ BRCA2/PALB2
P value Carriers Non-Carriers
Response to first taxane
PSA50 response rate (95%CI) 52·9% (29·2-76·6) 49·6% (43·8-55·6) 0·7920
ORR rate (95%CI) 30·0% (10·0-40·4) 14·7% (10·4-18·9) 0·1026
Response to first abi/enza
PSA50 response rate (95%CI) 44·4% (21·5-67·4) 53% (47·5-58·5) 0·4810
ORR rate (95%CI) 9·5% (0-2·7) 10·1% (6·7-22·2) 1.000
Outcomes BRCA2 carriers
P value Carriers Non-carriers
Response to first taxane
PSA50 response rate (95%CI) 45·5% (16·0-74·9) 50·0% (44·2-55·9) 0·7670
ORR rate (95%CI) 36·4% (7·9-64·8) 14·9% (10·7-19·1) 0·0764
Response to first abi/enza
PSA50 response rate (95%CI) 30% (1·6-58·4) 53·2% (47·8-58·6) 0·2020
ORR rate (95%CI) 16·7% (0-37·8) 9·8% (6·5-13·1) 0·3430
DNA REPAIR PATHWAY
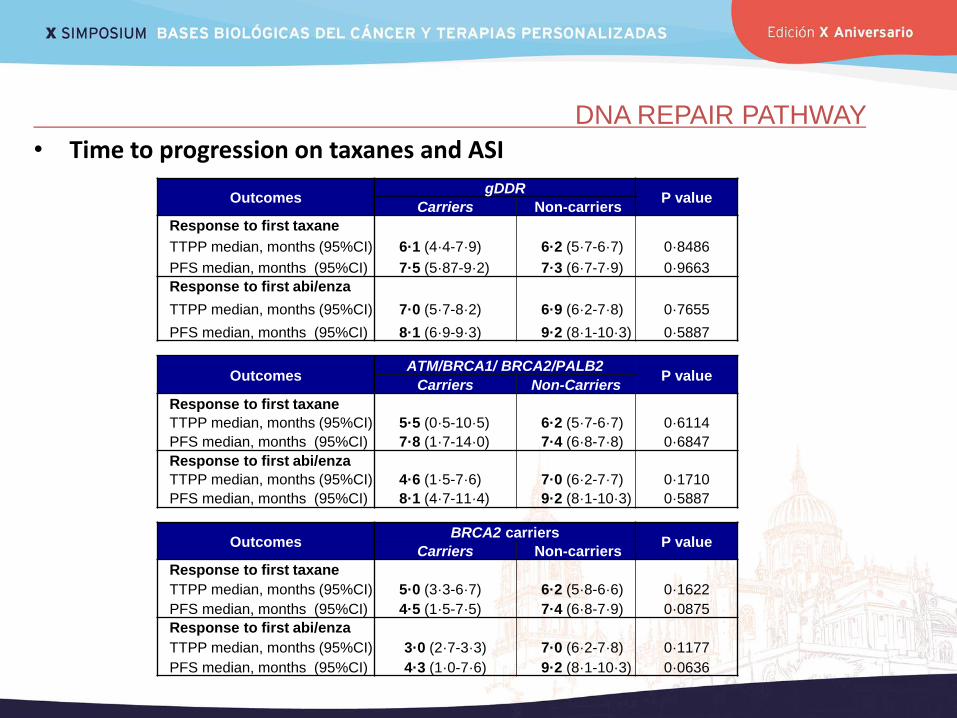
• Time to progression on taxanes and ASI
Outcomes gDDR
P value Carriers Non-carriers
Response to first taxane
TTPP median, months (95%CI) 6·1 (4·4-7·9) 6·2 (5·7-6·7) 0·8486
PFS median, months (95%CI) 7·5 (5·87-9·2) 7·3 (6·7-7·9) 0·9663
Response to first abi/enza
TTPP median, months (95%CI) 7·0 (5·7-8·2) 6·9 (6·2-7·8) 0·7655
PFS median, months (95%CI) 8·1 (6·9-9·3) 9·2 (8·1-10·3) 0·5887
Outcomes ATM/BRCA1/ BRCA2/PALB2
P value Carriers Non-Carriers
Response to first taxane
TTPP median, months (95%CI) 5·5 (0·5-10·5) 6·2 (5·7-6·7) 0·6114
PFS median, months (95%CI) 7·8 (1·7-14·0) 7·4 (6·8-7·8) 0·6847
Response to first abi/enza
TTPP median, months (95%CI) 4·6 (1·5-7·6) 7·0 (6·2-7·7) 0·1710
PFS median, months (95%CI) 8·1 (4·7-11·4) 9·2 (8·1-10·3) 0·5887
Outcomes BRCA2 carriers
P value Carriers Non-carriers
Response to first taxane
TTPP median, months (95%CI) 5·0 (3·3-6·7) 6·2 (5·8-6·6) 0·1622
PFS median, months (95%CI) 4·5 (1·5-7·5) 7·4 (6·8-7·9) 0·0875
Response to first abi/enza
TTPP median, months (95%CI) 3·0 (2·7-3·3) 7·0 (6·2-7·8) 0·1177
PFS median, months (95%CI) 4·3 (1·0-7·6) 9·2 (8·1-10·3) 0·0636
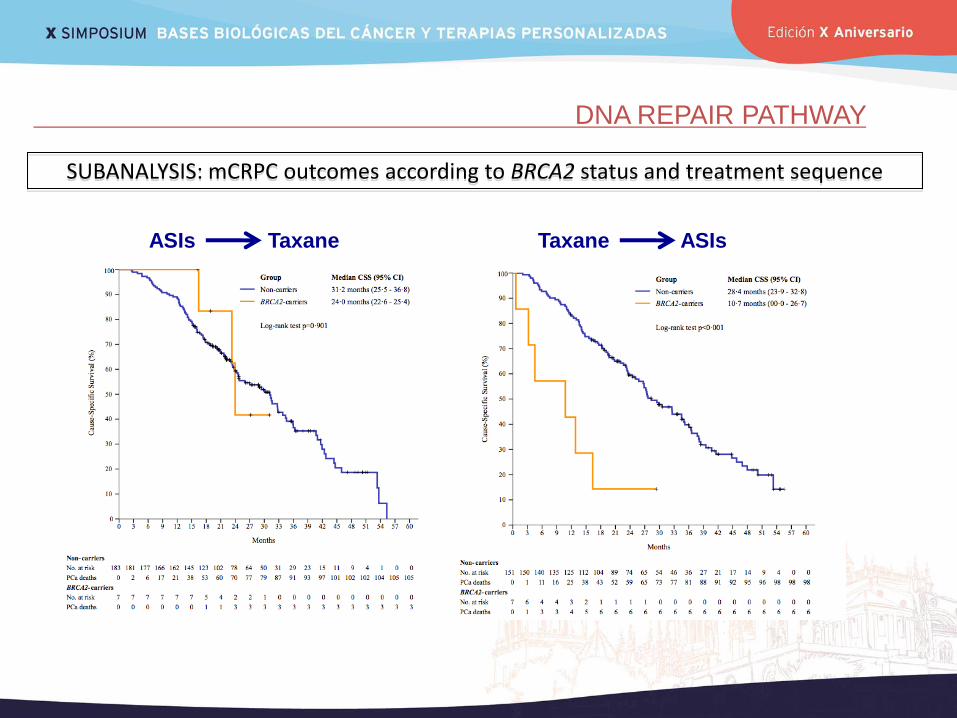
DNA REPAIR PATHWAY
ASIs Taxane Taxane ASIs
SUBANALYSIS: mCRPC outcomes according to BRCA2 status and treatment sequence
CONCLUSIONES
El cáncer de próstata es una enfermedad muy heterogénea, sin embargo, los avances acontecidos en la biología molecular nos están permitiendo obtener un mejor conocimiento y clasificación de esta entidad.
Importancia de los eventos policlonales en la evolución pronóstica del cáncer de próstata.
PSMA es una proteína transmembrana con prometedores resultados tanto en diagnóstico como en tratamiento.
Importancia de vía “DNA repair” en cáncer de próstata. Implicaciones terapéuticas y de screening genético.
PROREPAIR-B es el primer estudio que reporta prevalencia de mutaciones germinales en genes reparadores del ADN en una cohorte de pacientes con CPRCm mediterráneos.
Diferentes alteraciones en genes reparadores del ADN pueden tener diferente impacto en pacientes con CPRCm (BRCA2 peor pronóstico).
AGRADECIMIENTOS
PROREPAIR study investigators
Prostate Cancer Team at CNIO& IBIMA lead
by David Olmos & Elena Castro
Nuria Romero
Leticia Rivera
Gala Grau
Ylenia Cendón
Lorena Magraner
Visiting Researchers
Adriana Rosero
Ignacio Moreno
Isabel Santos
Collaborators at CNIO
Alicia Barroso
Ana Osorio
Antonio López
Berta Nasarre
Paz Nombela
Teresa Garcés
Vanessa Cañadilla
F. López-Campos
A.Gutierrez-Pecharromán
Jacobo Rogado
M. García-Ferrón
M. Ruiz-Vico
Noemí Hernández
INGEMM Pablo Lapunzina
Ángela del Pozo
Elena Vallespín
J.C. Silla-Castro
Kristina Ibáñez
Univ. of Washington Mallory Beightol
Colin Pritchard