Alineamiento Sagital Cervical

of 7
-
Upload
daniela-leyton-pezoa -
Category
Documents
-
view
214 -
download
0
Transcript of Alineamiento Sagital Cervical
-
7/29/2019 Alineamiento Sagital Cervical
1/7
SPINE Volume 33, Number 23, pp E870 E8762008, Lippincott Williams & Wilkins
Kinematic Analysis of the Relationship BetweenSagittal Alignment and Disc Degeneration in theCervical Spine
Masashi Miyazaki, MD,* Henry J. Hymanson, BS, Yuichiro Morishita, MD, PhD,
Wubing He, MD, Haihong Zhang, MD, Guizhong Wu, MD, Min Ho Kong, MD,
Hiroshi Tsumura, MD, PhD,* and Jeffrey C. Wang, MD
Study Design. Retrospective analysis using kinetic
magnetic resonance images (MRIs).
Objective. To investigate the relationship of changes in
the sagittal alignment of the cervical spine on the kinematics
of the functional motion unit and disc degeneration.
Summary of Background Data. Normal lordotic align-
ment is one of the most important factors contributing to
effective motion and function of the cervical spine. Loss
of normal lordotic alignment may induce pathologic
changes in the kinematics and accelerate degeneration ofthe functional motion unit. However, the relationship of
altered alignment on kinematics and degeneration has
not been evaluated.
Methods. Kinetic MRIs in flexion, neutral, and extension
were performed. Study participants were classified into 5
groups based on the C1C7 Cobb angle of sagittal align-
mentGroup A: Kyphosis (n 19), Group B: Straight (n
29), Group C: Hypolordosis (n 38), Group D: Normal (n
63), and Group E: Hyperlordosis (n 52).
Intervertebral disc degeneration was graded (Grades 15),
and the kinematics of the functional spinal unit were obtained.
Results. When the alignment shifted from normal to
less lordotic, the translational motion and angular varia-
tion tended to decrease at all levels. The contribution of
the C1C2, C2C3, and C3C4 levels to total angular mo-
bility tended to be higher in Group C than Group D. How-
ever, the contribution of the C4C5, C5C6, and C6C7
levels tended to be lower in Group C than in Group D. The
grade of disc degeneration associated with loss of lordo-
sis tended to be higher than that associated with normal
alignment at the C2C3 and C3C4 levels.
Conclusion. The present study demonstrated that the
changes in sagittal alignment of the cervical spine affect
the kinematics. Consequently, it may cause changes in
the segment subjected to maximum load for overall mo-
tion and accelerate its degeneration.
Key words: kinematic analysis, sagittal alignment, disc
degeneration, cervical spine, kinetic MRI. Spine 2008;33:
E870E876
The cervical spine withstands the axial load of thehead and is the most mobile region of the spine. Nor-mal lordotic alignment is one of the most importantfactors contributing to effective motion and functionof the cervical spine. The discs degenerate with age,and degeneration may ultimately affect the mechanicalproperties of spinal motion.1,2 On the other hand, itwas reported that severe degenerative changes tend to
produce less cervical lordosis.
3
The loss of normal lor-dotic alignment may induce pathologic changes in thekinematics and may accelerate degeneration of thefunctional motion unit. Furthermore, it is well knownthat sagittal malalignment in cervical degenerative dis-orders causes spinal morbidities such as neck pain anddeterioration of neurologic deficit.46 However, therelationship of altered alignment on the kinematicsand degeneration of the cervical spine has not beenelucidated thus far.
Kinetic magnetic resonance imaging (MRI) allows usto obtain images of patients in weight-bearing and flex-ion-extension positions and eventually provides consid-erable information, which would have been unavailableif a conventional MRI were used.2,711 It may also helpinunderstanding the true nature of spinal pathologies. Inaddition, it can demonstrate the mobility of each motionsegment and finally, relate the mobility to the changes insagittal alignment and disc degeneration.
The aim of this study was to investigate the relationshipbetween altered sagittal alignment of the cervical spine andthe kinematics of the functional motion unit and disc de-generation by using the kinetic MRI technology.
Materials and MethodsParticipants
From February 2006 to April 2007, kinetic MRI scans of thecervical spine were taken consecutively on 267 patients. Amongthese, 201 participants (90men and111 women) with mild symp-tomatic neck pain associated with movement, with/without radic-ulopathy or myelopathy, were included in this study. The meanageof the participants was 44 years (range, 1993 years). Patientswith recent trauma, rheumatoid arthritis, infectious spondylitis,spinal tumors, prior cervical fractures or dislocations, or priorcervical spine surgery were excludedfrom this study. Additionallyparticipants with severe neck pain who were expected to aggra-vate their symptoms by moving their neck or who were unable to
remain still during flexion-extension kinetic MRI scans were ex-cluded from this study.
From the *Department of Orthopaedic Surgery, Oita University, Oita,Japan. Department of Orthopaedic Surgery, University of Californiaat Los Angeles, Los Angeles, CA; and Department of Neurosurgery,Seoul Medical Center, Seoul, Korea.Acknowledgment date: March 7, 2008. Revision date: April 23, 2008.Acceptance date: May 16, 2008.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Jeffrey C. Wang, MD,Chief, Orthopaedic Spine Service, UCLA Comprehensive SpineCenter,1250 16th Street, Suite 745, Santa Monica, CA 90404; E-mail:[email protected]
E870
-
7/29/2019 Alineamiento Sagital Cervical
2/7
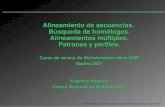
MRI PositioningParticipants were first seated on a bench between the two mag-nets in the neutral position with their heads facing straightahead without angling their chin up or down (0 neutral posi-tion) (Figure 1A). This positioning was used for the neutral
images. Next, the participants were positioned with their chinsangled toward their chests (40 flexion) (Figure 1B). This po-sitioning was used to obtain the flexion images. Finally, theparticipants were positioned with their chins angled towardsthe ceiling (20 extension) (Figure 1C). This positioning wasused to obtain the extension images. For each of these positionsa flexible cervical coil was placed around the participantsnecks and the front and back of their heads were supported andkept in place with a padded bar and a headrest. Their bodieswere not restricted by any fastening straps. Kinetic MRIs weretaken with both T1-weighted sagittal spin echo sequences andT2-weighted sagittal fast spin echo sequences in the neutralposition and T2-weighted sagittal fast spin echo sequences at
the cervical flexion and extension positions. Each of these se-quences took approximately 5 minutes to complete.
MRI TechniqueMRI of the cervical spine was performed using a 0.6 Tesla MRIscanner (UPRIGHT Multi-Position; Fonar Corp., NY, NY). Inthe MR unit, 2 doughnut-shaped magnets placed 18 inchesapart are vertically oriented, and this enables the scanning of apatient in an upright axially loaded position. Images were ob-tained using a flexible surface coil. We examined the T1-weighted sagittal spin echo images [repetition time, 671 milli-seconds; echo time, 17 milliseconds; thickness, 3.0 mm; field ofview, 24 cm; matrix, 256 200; and number of excitations(NEX), 2] and T2-weighted sagittal fast spin echo images (rep-etition time, 3432 milliseconds; echo time, 160 milliseconds;thickness, 3.0 mm; field of view, 24 cm; matrix, 256 224; andNEX, 2) of each patient.
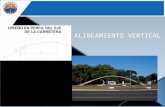
Study Groups Formed According to Sagittal AlignmentThe participants were classified into 5 groups based on theC1C7 Cobb angle of sagittal alignment observed on uprightneutral T2-imagesGroup A: Kyphosis (Cobb angle,0; n19); Group B: Straight (Cobb angle, 0to15; n 29); GroupC: Hypolordosis (Cobb angle, 15to 30; n 38); Group D:Normal (Cobb angle, 30to 45; n 63); Group E: Hyper-lordosis (Cobb angle, 45; n 52) (Figure 2).
Grades of Cervical Disc DegenerationA comprehensive grading system for cervical disc degenerationwas obtained using a previously reported system.2 Accord-
ingly, the neutral-position T2-weighted sagittal images of 1206
cervical intervertebral discs of the 201 subjects were classifiedinto 5 grades (Table 1) by the primary author and were judged
eligible for inclusion in the study.
Image AnalysisAll radiologic MRI data were recorded using computer-
based measurements, and all calculations were performedusing an MRI Analyzer (Truemetric Corp., Bellflower, CA),
as described previously.2 Sagittal MR images were analyzed
in 3 positionsflexion, neutral, and extension. For digitiza-
tion, 77 points were marked on each film by spine surgeons.Specific points were chosen for occiput (Oc), C1, and C2.
The anterior and posterior baselines were marked at the Oc.The anterior tubercle and the posterior margin of the atlasand the lowest end of the spinous process were marked atC1, and a point at the tip of the odontoid process was
marked at C2; other points were marked accordingly fromC3 to T1. For the typical cervical vertebrae from C3-T1, 4points were marked for the vertebral body (anterior-inferior,anterior-superior, posterior-superior, and posterior-inferiorjunctions); 2 points were marked for the disc height (themiddle of the endplate); and 2 points were marked for thepedicle and spinal cord diameters.
Basic measurements included all the static intervertebral an-gular displacements and translations calculated in differentpostures. Subsequently, total flexibility (motion segment integ-rity, translational motion, and angular variation) at each ver-tebral level was calculated from the difference between the flex-ion and extension positions. Translational motion was
measured for each segment at 5 cervical intervertebral disclevels, namely, C2C3, C3C4, C4C5, C5C6, and C6C7by determining the anteroposterior motion of 1 vertebra overthe other vertebra; a positive value implies anterior translation(antelisthesis), whereas a negative value implies posterior trans-lation (retrolisthesis). The sagittal angular variation was mea-sured for each segment at 5 cervical intervertebral disc levels,namely, C2C3, C3C4, C4C5, C5C6, and C6C7. For cal-culating angular variation, lines were drawn from the inferiorborders of the 2 vertebral bodies at a particular level. Thelordotic angle was defined as negative, whereas the kyphoticangle was defined as positive. In addition, the angular variationat the C1C2 level was calculated from the C1C7 Cobb angleand each individual angular variation.
To elucidate the mechanism underlying the changes in the roleof each cervical spine unit in flexion-extension motion depending
Figure 1. MRI positioning in neu-tral, flexion, and extension posi-tions. A, Neutral position. Partici-pants were first seated on a benchbetween the 2 magnets in a re-laxed position, with their headslooking straight ahead and withoutangling the chin (0 neutral posi-
tion). B, Flexion position. Partici-pants were positioned with theirschin angled toward their chests(40 flexion). C, Extension position.Participants were positioned withtheir chins angled toward the ceil-ing (20 extension).
E871Kinematic Analysis of Cervical Sagittal Alignment With Degeneration Miyazaki et al
-
7/29/2019 Alineamiento Sagital Cervical
3/7
on the changes in sagittal alignment, we calculated the contribu-tion of each level to the total angular mobility. The total sagittalmotionof thecervical spine wasdefined as theabsolute total of theindividualsagittal angularvariations (C1C2C2C3C3C4C4C5C5C6C6C7) in degrees. The contribution of each
segment to the total angular mobility of thecervicalspine betweenflexion and extension was defined as percentage segmental mobil-ity,which was calculated as follows:(thesagittalangular variationof each segment in degrees)/(total sagittal angular motion in de-grees) 100.
Figure 2. Study Groups accord-ing to sagittal alignment. A,Group A: Kyphosis (Cobb angle,0). B, Group B: Straight (Cobbangle, 0 to 15). C, Group C:Hypolordosis (Cobb angle, 15to30). D, Group D: Normal (Cobbangle, 30 to 45). E, Group E:Hyperlordosis (Cobb angle,45).
Table 1. Grading System for Cervical Intervertebral Disc Degeneration
Grade Nucleus Signal Intensity Nucleus Structure Distinction of Nucleus and Annulus Disc Height
I Hyperintense Homogenous, white Clear NormalII Hyperintense Inhomogenous with horizontal band, white Clear NormalIII Intermediate Inhomogenous, gray to black Unclear Normal to decreased
IV Hypointense Inhomogenous, gray to black Lost Normal to decreasedV Hypointense Inhomogenous, gray to black Lost Collapsed
E872 Spine Volume 33 Number 23 2008
-
7/29/2019 Alineamiento Sagital Cervical
4/7
Statistical AnalysisThe SPSS software (version 13; SPSS, Chicago, IL) was used,and the values are represented as mean standard deviation(SD). Student t test was used for statistical analysis. A signifi-cance level of 0.05 was adopted.
Results
Comparison of Each Group in the Study PopulationThe number, gender distribution, and age of the partici-pants are shown in Table 2. There were no statisticaldifferences among the groups.
General Trends in ResultsWhen normal lordotic alignment progressed to hypolor-dotic alignment and straight alignment, all levels of thecervical spine tended to have decreased translationalmotion and angular variation. Although angular vari-ation decreased at all levels, the percent contributionto total angular variation of the upper (C2C3, C3C4) levels tended to increase. In contrast, the percentcontribution to total angular variation of the middle(C4C5, C5C6) and low (C6C7) levels tended todecrease. Additionally, this change in alignment wasassociated with increased grades of disc degenerationat the upper levels. However, there were no significant
associations observed between this alignment shift andthe grade of disc degeneration at the middle and lowlevels. When alignment shifted from normal lordosisto hyperlordosis, translational motion, angular varia-tion, and the percent contribution to total angularvariation at the middle levels increased. However,these changes in mobility had no significant effects ondisc degeneration. At the upper levels, translational
motion decreased in participants with hyperlordoticalignments. Additionally, the grade of disc degenera-tion at the upper levels was lower in participants withhyperlordotic alignment when compared with partic-ipants with normal lordotic alignment.
The Correlation Between the Sagittal Alignmentand the Degree of Cervical Disc Degeneration
The grades of disc degeneration in each group areshown in Figure 3. In all the groups, maximum degen-eration was noted at the intervertebral disc at theC5C6 level followed by that at the C4C5 level. At
the C3C4 level, the grade of disc degeneration washigher in Group B than in Group D and was lower inGroup E than in Group D. Further, at the C2C3 level,the grade of disc degeneration in Group E was signif-icantly lower than that in Group D (P 0.05). Inter-estingly, the grade of disc degeneration at the C5C6level in Group A was significantly higher than that inGroup D (P 0.05).
Translational Motion of Each Cervical UnitFigure 4 presents the graphs of translational motion of eachcervical unit. At the C4C5 and C5C6 levels, the transla-tional motion in Group E tended to be higher than that in
Group D; however, the translational motion was lower inGroup C and Group B than in Group D, whereas it waslower in Group B than in Group C. At the C2C3 andC3C4 levels, the translational motion in Group E tendedto be lower than that in Group D. There were significantdifferences between Group E and Group D at the C2C3and C5C6 levels (P 0.05). At all the levels, the transla-tional motion in Group C and Group B was lower than that
Figure 3. The Correlation be-tween the sagittal alignment andthe degree of cervical disc de-generation. At the C3C4 level,the grade of disc degenerationwas higher in Group B than inGroup D and was lower in GroupE than in Group D. Further, at theC2C3 level, the grade of discdegeneration in Group E was sig-nificantly lower than that inGroup D (P 0.05). The grade ofdisc degeneration at the C5C6level in Group A was significantlyhigher than that in Group D (P0.05).
Table 2. Comparison of Each Group in the Study Population
(Group) A: Kyphosis B: Straight C: Hypolordosis D: Normal E: Hyperlordosis
No. 19 29 38 63 52Sex (female/male) 13/6 14/15 24/14 35/28 25/27Age 46.0 13.6 41.0 12.0 42.6 11.4 43.2 9.3 45.4 14.4
E873Kinematic Analysis of Cervical Sagittal Alignment With Degeneration Miyazaki et al
-
7/29/2019 Alineamiento Sagital Cervical
5/7
in Group D. In Group A, the translational motion at theC5C6 level was the lowest, whereas that at the C3C4,C4C5, and C6C7 levels was definitely higher. Therewere significant differences between Group A and Group Dat the C2C3 level (P 0.05).
Angular Variation of Each Cervical UnitFigure 5 shows the graphs of angular variation of eachcervical unit. At the C4C5 and C5C6 levels, the angu-lar variation tended to be higher in Group E than inGroup D. However, at the same level, the angular vari-
ation was lower in Groups C and B than in Group D andit was lower in Group B than in Group C. There weresignificant differences between Group E and Group Dwith regard to the angular variation at the C5C6 leveland between Group B and Group D with regard to thevariation at the C4C5 level (P 0.05).
Contribution of Each Level to Total Angular Mobility
The contribution of each level to the total angular mobilityis shown in Figure 6. The contribution of the C4C5 andC5C6 levels to the total angular mobility tended to be
higher in Group E than in Group D. However, at the C4C5,C5C6, and C6C7 levels, the total angular mobility inGroup C and Group B was lower than that in Group D,
whereas it was lower in Group B than in Group C. Therewere significant differences between Group E and Group D
at the C5C6 level (P 0.05). The contribution of theC1C2, C2C3, and C3C4 levels to the total angularmobility tended to be higher in Group C and Group B
than in Group D, whereas it tended to be higher inGroup B than in Group C. There were significant dif-ferences between Group B and Group D at the C2C3
level (P 0.05).
Figure 4. Translational motion ofeach cervical unit. There weresignificant differences betweenGroup E and Group D at theC2C3 and C5C6 levels and be-tween Group A and Group D atthe C2C3 level (P 0.05).
Figure 5. Angular variation ofeach cervical unit. There weresignificant differences betweenGroup E and Group D with regardto the angular variation at theC5C6 level and between GroupB and Group D with regard to thevariation at the C4C5 level (P0.05).
E874 Spine Volume 33 Number 23 2008
-
7/29/2019 Alineamiento Sagital Cervical
6/7
Discussion
The cervical spine withstands substantial compressiveaxial load, which is approximately thrice the weight ofthe head because of muscle coactivation forces function-ing to balance the head in the neutral position.12 Thecompressive force increases during flexion and extensionand other routine movements. Cervical lordosis is con-sidered to decrease the internal compressive load and isessential for appropriate spinal coupling motion.1315
A major portion of this axial load is sustained by the
intervertebral discs.
16
During physiologic aging, degen-erative changes are noted in many discs at around middleage. The changes usually occur gradually, and some in-dividuals experience neck symptoms because of cervicaldegenerative disorders. The degeneration affects the mo-tion units and the overall kinematics of the cervicalspine,1,2 and axial loading is negatively affected. Thismay lead to the loss of normal cervical lordosis and con-siderable acceleration of the degeneration process.
There are a few reports on the correlation of alignmentand the kinematics of the cervical spine. Takeshima et alinvestigated the association between sagittal cervical kine-matics and changes in the static alignment on upright cer-vical lordosis by using conventional lateral radiographs;they concludedthat alterations in thestatic alignmentof thecervical curvature causes alterations in the dynamic kine-matics of the cervical spine during the flexion-extensionmotion.17 However, they did not comment on the relation-ship of degeneration on the changes in kinematics.
In the present study, we observed that the translationalmotion and angular variation in Group E was greater thanthat in Group D at the C4C5 and C5C6 levels, whichwas the apex of the lordosis. Further, the contribution ofeach of these levels to the total angular mobility in Group Etended to be higher than that in Group D. Moreover, at the
C2C3 level, the translational motion in Group E waslower than that in Group D. At the C2C3 and C3C4
levels, and disc degeneration in Group E was lower thanthat in Group D. It was assumed that a shift from normallordosis to hyperlordosis renders the segment correspond-ing to the tip of lordosis more mobile and that this segmentplays a major role in the total mobility during flexion-extension motions; moreover, such an alteration in align-ment accelerates degeneration of this segment rather thanthat of other parts.
Furthermore, translational motion and angular vari-ation tended to decrease when normal lordotic alignmentchanged to loss of lordosis or straight alignment at all
levels, i.e., when the cervical spine became more rigid.Disc degeneration was greater in Group B than in GroupD at the C2C3 and C3C4 levels, and the contributionof C1C2, C2C3, and C3C4 levels in Group C andGroup B tended to be higher than that in Group D. Incontrast, the contribution of the C4C5, C5C6, andC6C7 levels in Group C and Group B tended to belower than that in Group D.
A limitation of our study was that we could not evaluatekyphotic or sigmoid (local kyphosis) cervical spines in de-tail because the number of participants with these align-ments was less. Interestingly, we observed that the grade ofdisc degeneration at the C5C6 level in Group A was sig-nificantly greater than that in Group D; the translationalmotion at the C5C6 level was the lowest among all func-tional motion units; and the translational motion at theC3C4, C4C5, and C6C7 levels was definitely higherthan that at the C5C6 level. It was obvious that the kine-matics in Group A lost the physiologic principle. Based onthese results, it wasassumed that thefunctional motion unitat the C5C6 level became more rigid and ankylosed, andthe adjacent or 2 adjacent functional motion units becamemore mobile.
The correlation between the cervical normal sagittal
alignment and clinical symptoms is controversial becausesmall segmental kyphotic regions have been detected in
Figure 6. Contribution of eachlevel to total angular mobility.There were significant differ-ences between Group E andGroup D at the C5C6 level andbetween Group B and Group D atthe C2C3 level (P 0.05).
E875Kinematic Analysis of Cervical Sagittal Alignment With Degeneration Miyazaki et al
-
7/29/2019 Alineamiento Sagital Cervical
7/7
asymptomatic subjects.3,18,19 However, the incidence ofsegmental kyphosis is reported to be more than 4 times
greater in patients with neck pain than in asymptomaticsubjects.3,19,20 Further, we have experienced that mainte-nance of cervical lordosis after surgery is very important for
preventing the recurrence of symptoms.46,21,22 However,the concept that the loss of cervical lordosis accelerates de-
generation and causes symptoms has not yet been eluci-dated. Katsuuraetalreportedthatdegeneration of adjacentcervical levels was significantly associated with the loss of
physiologic cervical lordosis in a retrospective study of pa-tients who had undergone anterior cervical discectomy andfusion.23 The present study demonstrated that the changes
in the sagittal alignment of the cervical spine affects thekinematics and the contribution of each segment to thetotal angular mobility. Consequently, it may cause
changes in the segment bearing the major load foroverall motion and accelerate its degeneration. As in-ferred from a clinical case series study,23 we should
consider physiologic lordotic reconstruction for pre-venting degeneration and symptomatic deterioration
while planning cervical surgeries such as anterior cer-vical discectomy and fusion or artificial disc replace-ment.
In conclusion, the present study demonstrated a cor-relation between disc degeneration and static sagittalalignment of the cervical spine. We analyzed the changes
in the kinematics of the functional motion unit accordingto the different types of cervical sagittal alignments. Our
results suggest that a change in the sagittal alignment of
the cervical spine affects the kinematics and the progressof degeneration in the cervical spine. Nevertheless, we
investigated these analyses retrospectively and not pro-spectively. Therefore, further prospective researches arerequired to elucidate the details of the natural history ofcervical spine degeneration. Further studies are requiredto provide with appropriate treatments for cervical de-generative disease.
Key Points
The present study investigated the correlation
between disc degeneration and static sagittal align-ment of the cervical spine and the changes in thekinematics of the functional motion unit accordingto different types of sagittal alignment. Thepresent study demonstrated that the changes insagittal alignment of the cervical spine affects the ki-nematics and the contribution of each segment to thetotal angular mobility. Consequently, it may causechanges in the segment subjected to maximum loadfor overall motion and accelerate its degeneration.
From the results of the present study, cervicalsurgery such as cervical discectomy and fusion orartificial disc replacement should attempt to restorelordosis to prevent degeneration and symptomaticdeteriorations.
References
1. Dai L. Disc degeneration and cervical instability. Correlation of magnetic
resonance imaging with radiography. Spine 1998;23:17348.
2. Miyazaki M, Hong SW, Yoon SH, et al. Kinematic analysis of the relation-
ship between the grade of disc degeneration and motion unit of the cervical
spine. Spine 2008;33:18793.
3. Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical
spine in asymptomatic people. Spine 1986;11:5214.
4. Suda K, Abumi K, Ito M, et al. Local kyphosis reduces surgical outcomes of
expansive open-door laminoplasty for cervical spondylotic myelopathy.
Spine 2003;28:125862.
5. Barsa P, Suchomel P. Factors affecting sagittal malalignment due to cage
subsidence in standalone cage assisted anterior cervical fusion. Eur Spine J
2007;16:1395400.
6. Kawaguchi Y, Kanamori M, Ishihara H, et al. Minimum 10-year fol-
lowup after en bloc cervical laminoplasty. Clin Orthop Relat Res 2003;411:12939.
7. Schlamann M, Reischke L, Klassen D, et al. Dynamic magnetic resonance
imaging of the cervical spine using the NeuroSwing System. Spine 2007;32:
2398401.
8. Kuwazawa Y, Pope MH, Bashir W, et al. The length of the cervical cord:
effects of postural changes in healthy volunteers using positional magnetic
resonance imaging. Spine 2006;31:E57983.
9. Kuwazawa Y, Bashir W, Pope MH, et al. Biomechanical aspects of the
cervical cord: effects of postural changes in healthy volunteers using posi-
tional magnetic resonance imaging. J Spinal Disord Tech 2006;19:34852.
10. Hirasawa Y, Bashir WA, Smith FW, et al. Postural changes of the dural sac
in the lumbar spines of asymptomatic individuals using positional stand-up
magnetic resonance imaging. Spine 2007;32:E13640.
11. Gupta V, Khandelwal N, Mathuria SN, et al. Dynamic magnetic resonance
imaging evaluation of craniovertebral junction abnormalities. J Comput As-
sist Tomogr 2007;31:3549.12. Moroney SP, Schultz AB, Miller JA. Analysis and measurement of neck
loads. J Orthop Res 1988;6:71320.
13. Patwardhan AG,Havey RM, Ghanayem AJ, et al.Load-carrying capacity of
the human cervical spine in compression is increased under a follower load.
Spine 2000;25:154854.
14. Panjabi MM, Oda T, Crisco JJ III, et al. Posture affects motion coupling
patterns of the upper cervical spine. J Orthop Res 1993;11:52536.
15. Penning L, Wilmink JT.Rotation of thecervical spine. A CT study in normal
subjects. Spine 1987;12:7328.
16. Broberg KB. On the mechanical behaviour of intervertebral discs. Spine
1983;8:15165.
17. Takeshima T, Omokawa S, Takaoka T, et al. Sagittal alignment of cer-
vical flexion and extension: lateral radiographic analysis. Spine 2002;27:
E34855.
18. Gay RE. The curve of the cervical spine: variations and significance. J Ma-
nipulative Physiol Ther 1993;16:5914.19. Hardacker JW, Shuford RF, Capicotto PN, et al. Radiographic standing
cervical segmental alignment in adult volunteers without neck symptoms.
Spine 1997;22:147280.
20. McAviney J, Schulz D, Bock R, et al. Determining the relationship between
cervical lordosis and neck complaints.J Manipulative Physiol Ther 2005;28:
18793.
21. Suk KS, Kim KT, Lee JH, et al. Sagittal alignment of the cervical spine after
the laminoplasty. Spine 2007;32:E65660.
22. Kim SW, Shin JH, Arbatin JJ, et al. Effects of a cervical disc prosthesis on
maintaining sagittal alignment of the functional spinal unit and overall sag-
ittal balance of the cervical spine. Eur Spine J2008;17:209.
23. Katsuura A, Hukuda S, Saruhashi Y, et al. Kyphotic malalignment after
anterior cervical fusion is one of the factors promoting the degenerative
process in adjacent intervertebral levels. Eur Spine J2001;10:3204.
E876 Spine Volume 33 Number 23 2008