11 Fang Atrial Fib - UCSF CME · 10/9/15 1 MargaretC.Fang,MD,MPH! AssociateProfessorofMedicine,’...
24
10/9/15 1 Margaret C. Fang, MD, MPH Associate Professor of Medicine, Division of Hospital Medicine Medical Director, UCSF Anticoagulation Clinic No financial conflicts of interest Member of the ABIM FocusedPractice in Hospital Medicine Self Examination Process committee No exam questions will be disclosed in the presentation
Transcript of 11 Fang Atrial Fib - UCSF CME · 10/9/15 1 MargaretC.Fang,MD,MPH! AssociateProfessorofMedicine,’...

10/9/15
1
Margaret C. Fang, MD, MPH
� Associate Professor of Medicine, Division of Hospital Medicine
� Medical Director, UCSF Anticoagulation Clinic
� No financial conflicts of interest � Member of the ABIM Focused-‐Practice in Hospital Medicine Self Examination Process committee � No exam questions will be disclosed in the presentation

10/9/15
2
Case Presenta0on � A 67 year old woman comes to you for a routine visit � Past medical history: only notable for hypertension
� Meds: metoprolol 50 mg BID � Exam:
� BP 120/80 � Irregularly irregular heart rate � No signs or symptoms of heart failure
� EKG: atrial fibrillation, rate of 97 � Symptoms: none; no palpitations, dizziness.
Case � You diagnose her with atrial fibrillation
� In between counseling her on age-‐appropriate cancer screening, updating her vaccinations, and advising her on diet, activity, and osteoporosis prevention, you talk about this new diagnosis with her.

10/9/15
3
Session Objec0ves � To review key updates in the management of AF � Help you understand how to choose an appropriate anticoagulant for your patient with AF
� Review the latest evidence for perioperative bridging in patients with AF
Guideline Recommenda0ons 1. Rate control 2. Rhythm control 3. Preventing thromboembolism
2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation, Circulation 2014; 129

10/9/15
4
Strength of Recommenda0ons: Class and Level of Evidence � Size of Treatment Effect
� Class I: you SHOULD do it (benefit >>> risk) � Class IIa: it is REASONABLE to do it (benefit >> risk) � Class IIb: may CONSIDER doing it (benefit ≥ risk) � Class III: no benefit or harm
� Quality of the evidence � Level A: strong evidence, multiple populations � Level B: moderate evidence, limited populations � Level C: weak evidence, very limited populations
Ini0al Clinical Evalua0on � Establish the diagnosis of AF using ECG (Class IC) � Characterize the type of AF and assess symptom burden
� Treat associated medical conditions � CHF, hypertension
� Transthoracic echocardiogram to detect underlying cardiac disease, evaluate cardiac function, and measure left atrial size
� Other tests as appropriate � Sleep study, thyroid evaluation, pulmonary evaluation

10/9/15
5
Q1: Rate control She is on metoprolol 50mg BID. Her resting HR is 97. What do you do for rate control?
1. Continue metoprolol at current dose 2. Increase her metoprolol dose 3. Change metoprolol to diltiazem 4. Add digoxin
Q1: Rate control She is on metoprolol 50mg BID. Her resting HR is 97. What do you do for rate control?
1. Continue metoprolol at current dose 2. Increase her metoprolol dose 3. Change metoprolol to diltiazem 4. Add digoxin

10/9/15
6
Rate Control for AF
Rate Control � Control the ventricular rate (Class I) � Target heart rates
� < 80 bpm for symptomatic patients (Class IIaB) � < 110 if asymptomatic and no heart failure (Class IIbB)

10/9/15
7
How to Rate Control � Medications
� Beta-‐blocker (Class IB) � Nondihydropyridine calcium channel blocker (Class IB) � Amiodarone (if failed other measures, Class IIbC)
� AV nodal ablation + permanent ventricular pacing if pharmacologic therapy is inadequate and rhythm control unachievable (Class IIaB)
Rate Control for Atrial Fibrillation
No other CV disease LV dysfunction or
HF Hypertension or
HFpEF
Beta blocker Diltiazem Verapamil
Beta blocker Diltiazem Verapamil
Beta blocker Digoxin
Amiodarone

10/9/15
8
Don’t Dos � Don’t use AV nodal ablation/pacing without an adequate trial of medications (Class IIIC-‐harm)
� Don’t use nondihydropyridine CCBs in patients with decompensated CHF (Class IIIC-‐harm)
� Don’t use digoxin, nondihydropyridine CCBs, or IV amiodarone in patients with pre-‐excitation and AF (increases risk of VFib) (Class IIIB-‐harm)
� Don’t use dronedarone as rate control in patients with permanent AF (Class IIIB-‐harm)
Rhythm Control for AF

10/9/15
9
Rhythm Control � May be appropriate in symptomatic patients � Options include antiarrhythmic drugs and catheter ablation
� Treat reversible causes prior to initiating antiarrhythmic drugs (Class IC)
An0arrhythmic Drugs � Recommended for treating tachycardia-‐induced cardiomyopathy (Class IIaC)
� Consider if there are infrequent, well-‐tolerated episodes of AF and treatment reduces symptoms/frequency (Class IIbC)
� Discontinue if AF becomes permanent (Class IIIB-‐harm)
� Risks of antiarrhythmic drugs should be considered prior to initiating therapy (Class IC)

10/9/15
10
An0arrhythmic Drugs � Dofetilide � Flecainide � Propafenone � Sotalol � Amiodarone
� Should be used only if risks/side effects are considered and other agents are not suitable (Class IC)
� Dronedarone � Don’t use in heart failure (Class IIIB-‐harm)
Catheter Abla0on � May be useful for symptomatic patients who do not tolerate or have failed antiarrhythmic medications (Class IA) � Might be a reasonable initial strategy in some patients
� Need to assess procedural risks and outcomes relevant to your individual patient (Class IC)
� Does not obviate the need for anticoagulation � Should not be performed in patients who cannot be treated with anticoagulants periprocedurally (Class IIIC-‐harm)

10/9/15
11
Catheter Abla0on � Consider for patients with symptomatic paroxysmal or persistent AF as an initial strategy, or who are refractory or intolerant to antiarrhythmic drugs
� Consider for symptomatic long-‐standing persistent AF (>12 mo) if refractory or intolerant to meds
Rhythm Control AF without structural heart
disease
Dofetilide Dronedarone Flecainide
Propafenone Sotalol
Catheter ablation
Amiodarone

10/9/15
12
Rhythm Control AF with structural heart disease
CAD Heart Failure
Dofetilide Dronedarone
Sotalol Catheter ablation
Amiodarone Dofetilide
Amiodarone
Preven0on of Thromboembolism

10/9/15
13
Q2: Es0ma0ng stroke risk Your patient is 67 and has a history of hypertension. No history of stroke or other cardiovascular disease. What is her annual risk for stroke?
1. <1 % 2. 3% 3. 8% 4. >10%
Q2: Es0ma0ng stroke risk Your patient is 67 and has a history of hypertension. No history of stroke or other cardiovascular disease. What is her annual risk for stroke?
1. <1 % 2. 3% 3. 8% 4. >10%

10/9/15
14
Preven0ng Thromboembolism � It doesn’t matter if the AF is paroxysmal, persistent, or permanent à stroke prevention is the same (Class IB)
� Individualize decision-‐making on antithrombotic therapy based on stroke risk, bleeding risk, and patient’s values and preferences (Class IC)
� Periodically re-‐evaluate need and choice of antithrombotic therapy (Class IC)
Es0mate Stroke Risk � Previous recommendation used CHADS2 risk score � Updated recommendations now recommend the CHA2DS2-‐VASc score (Class IB)

10/9/15
15
CHA2DS2-‐VASc
Risk Factor Score Congestive heart failure 1 Hypertension 1 Age ≥75 years 1 Diabetes 1 Stroke 2
Risk Factor Score Congestive heart failure 1 Hypertension 1 Age ≥75 years 2 Diabetes 1 Stroke 2 Vascular disease (MI, peripheral arterial disease, aortic atherosclerosis) 1 Age 65-‐74 years 1 Sex category (female) 1
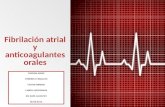
CHADS2
0 2 4 6 8 10 12 14 16 18 20
0 1 2 3 4 5 6 7 8 9
Annual Stroke Rate(%)
CHADS2 CHA2DS2-‐VASc
Score
CHADS2 = 1
CHA2DS2-‐VASc = 3
An0thrombo0c Therapy CHA2DS2-‐VASc Score Recommendation
0 No antithrombotic therapy (Class IIaA)
1 No antithrombotic therapy vs. Aspirin vs.
Oral anticoagulant (Class IIbC)
2 or higher Oral anticoagulant (Class IA)

10/9/15
16
Q3: What an0coagulant do you choose? Your patient’s CHA2DS2-‐VASc score is 3 and guidelines recommend chronic anticoagulation. Which of the following will you choose? 1. Warfarin, target INR 2-‐3 2. Dabigatran (Pradaxa®) 150mg BID 3. Rivaroxaban (Xarelto®) 20mg daily 4. Apixaban (Eliquis®) 5mg BID 5. Edoxaban (Savaysa®) 60mg daily 6. It depends!
Q3: What an0coagulant do you choose? Your patient’s CHA2DS2-‐VASc score is 3 and guidelines recommend chronic anticoagulation. Which of the following will you choose? 1. Warfarin, target INR 2-‐3 2. Dabigatran (Pradaxa®) 150mg BID 3. Rivaroxaban (Xarelto®) 20mg daily 4. Apixaban (Eliquis®) 5mg BID 5. Edoxaban (Savaysa®) 60mg daily 6. It depends!

10/9/15
17
Choice of An0coagulants � In patients with a mechanical heart valve, use warfarin (Class IB)
� In patients with nonvalvular AF who need anticoagulation: � Warfarin (Class IA)– OR – a non-‐vitamin K oral anticoagulant (Class IB)
� Direct thrombin inhibitor: dabigatran � Factor Xa inhibitors: rivaroxaban, apixaban, edoxaban
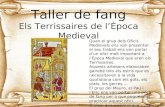
NOACs vs. Warfarin in AF
Ruff CT et al. Lancet 2014
ICH GI bleed
Ischemic stroke

10/9/15
18
Non-‐Vitamin K Oral An0coagulants � Consider if unable to maintain therapeutic INRs on warfarin (Class IC)
� Monitor renal function before initiating and periodically afterwards (Class IB)
� Reduced dosing might be considered for patients with moderate to severe renal disease (Class IIbC)
� Not recommended for patients with end stage kidney disease (Class IIIC-‐no benefit)
� Don’t use in patients with mechanical heart valves (Class IIIB-‐harm)
How to Choose? NOACs Warfarin RR
Ischemic stroke Same 0.92 (0.83-‐1.02)
ICH NOACs better 0.48 (0.39-‐0.59)
GI bleeding NOACs worse 1.25 (1.01-‐1.55)
Mortality NOACs better 0.90 (0.85-‐0.95)
Dosing Fixed dosing Adjusted dosing
Adherence Very important Very important
Monitoring No Yes
Interactions Fewer Many
Cost High Low
Reversibility Not proven Yes
Special concerns Renal, liver Liver
Ruff CT et al. Lancet 2014

10/9/15
19
Available Oral An0coagulants for AF Monitoring Drug interactions Dosing Reversal
Warfarin Coumadin®
INR Many Adjusted to INR 2-‐3 Vit K, FFP, PCC
Dabigatran Pradaxa®
None (thrombin time*)
P-‐gp inducers (rifampin), inhibitors
(ketoconazole, amiodarone)
150mg BID 75mg BID if CrCL 15-‐30
?
Rivaroxaban Xarelto®
None (Anti-‐Xa level*) CYP3A4/P-‐gp inducers
(carbamezepine, phenytoin, rifampin) Strong CYP3A4/P-‐gp inhibitors (protease
inhibitors, ketoconazole, clarithromycin)
20mg daily 15 mg daily if CrCl 15-‐50
?
Apixaban Eliquis®
None (Anti-‐Xa level*)
5mg BID 2.5mg BID if 2 of
following (age ≥80, wt < 60kg, Cr≥1.5)
?
Edoxaban Savaysa®
None (Anti-‐Xa level*)
P-‐gp inducers (rifampin)
60mg daily 30mg daily if CrCl 15-‐50 Do not use if CrCl>95
?
*normal value excludes clinically significant effect
Non-‐an0coagulant means to prevent stroke � Left atrial appendage closure (Watchman™ device)
� Could be considered in people who cannot take anticoagulants
� Invasive, periprocedural risks � Trials only included people who were candidates for anticoagulation � Anticoagulated for the first ~45 days after implantation

10/9/15
20
LAA Closure vs. Warfarin: Efficacy and Safety
Reddy VY et al. JAMA 2014
Case -‐ con0nued � After an extensive discussion on the pros and cons of different options, your patient decides to take warfarin.
� Over the past year, she has tolerated warfarin well with no side-‐effects and good INR control
� Her health has otherwise been good but she is scheduled for a colonoscopy. Her gastroenterologist asks that her anticoagulation be fully held for the procedure.
� Your patient’s weight is 60kg and her renal function is normal.

10/9/15
21
Q4: What is your periprocedural recommenda0on?
WARFARIN Pre-‐procedure BRIDGING
Post-‐procedure BRIDGING
1 Hold 5 days None Restart warfarin, no bridging
2 Hold 5 days Enoxaparin 40mg daily Restart warfarin Enoxaparin 40mg daily until INR 2-‐3
3 Hold 5 days Enoxaparin 120mg Q12 Restart warfarin, no bridging
4 Hold 5 days Enoxaparin 120mg Q12 Restart warfarin, Enoxaparin 120mg Q12 until INR 2-‐3
Q4: What is your periprocedural recommenda0on?
WARFARIN Pre-‐procedure BRIDGING
Post-‐procedure BRIDGING
1 Hold 5 days None Restart warfarin, no bridging
2 Hold 5 days Enoxaparin 40mg daily Restart warfarin Enoxaparin 40mg daily until INR 2-‐3
3 Hold 5 days Enoxaparin 120mg Q12 Restart warfarin, no bridging
4 Hold 5 days Enoxaparin 120mg Q12 Restart warfarin, Enoxaparin 120mg Q12 until INR 2-‐3

10/9/15
22
Should you bridge for AF?
No Bridging Bridging P value
Arterial thromboembolism (stroke/TIA/peripheral embolism)
0.4% 0.3% 0.73
Major bleeding 1.3% 3.2% 0.005
Minor bleeding 12% 21% <0.001
Death 0.5% 0.4% 0.88
� BRIDGE Trial: randomized 1813 patients with AF to perioperative bridging vs. no bridging
� Mean CHADS2 = 2.3 (only 3% had CHADS2 5-‐6)
� Bridging not beneficial (and actually harmful) for AF � But might consider for patients at high stroke risk
Douketis JD et al. NEJM 2015
Periprocedural management of NOACs � NOACs have faster off-‐set than warfarin
� Bridging generally not recommended � Need to consider half-‐life of the medication as well as renal function and risk of the procedure
� After the procedure, restart NOAC once bleeding risk is acceptable � Full anticoagulation effect within hours

10/9/15
23
Drug
Renal Function
Pre-procedure management Last Dose of Anticoagulant
Low Bleeding Risk Procedure High Bleeding Risk Procedure
Dabigatran CrCl > 50 ml/min T1/2= 12-17 h 2 days before surgery 3 days before surgery
CrCl 30-50 ml/min T1/2= 16-18 h 3 days before surgery 4-5 days before surgery
CrCl 15-30 ml/min T1/2 = 27 hrs 4-5 days before surgery 5-6 days before surgery
Rivaroxaban CrCl > 50 ml/min T1/2= 8-9 h 2 days before surgery 3 days before surgery
CrCl 30-50 ml/min T1/2= 9 h 2 days before surgery 3 days before surgery
CrCl 15-29.9 ml/min T1/2=9-10.5 h 3 days before surgery 4 days before surgery
Apixaban CrCl > 50 ml/min T1/2= 7-8 h 2 days before surgery 3 days before surgery
CrCl 30-50 ml/min T1/2= 17-18 h 3 days before surgery 4 days before surgery
Edoxaban
CrCl > 50 ml/min T1/2= 10-14 h 2 days before surgery 3 days before surgery
NOACs: Suggested Periprocedural Management
Drug
Post-procedure management
Low Bleeding Risk Procedure High Bleeding Risk Procedure
Dabigatran
Resume 24 hours post-procedure
Resume 48-72 hours post-procedure
In patients with very high thrombotic risk, can consider using prophylactically-dosed LMWH at 24 hours and until NOAC is restarted
Rivaroxaban
Apixaban
Edoxaban
NOACs: Periprocedural Management

10/9/15
24
Summary of Key Points � HR control <80 if symptomatic, <110 if asymptomatic and no CHF
� Catheter ablation can be considered for symptomatic patients
� Use CHA2DS2-‐VASc score to determine stroke risk and need for anticoagulation
� Several choices for oral anticoagulation in AF; choose based on clinical factors, renal function, preference, and cost
� Periprocedural bridging has no benefit in AF patients with low-‐moderate stroke risk and caused harm
Thank you!